This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
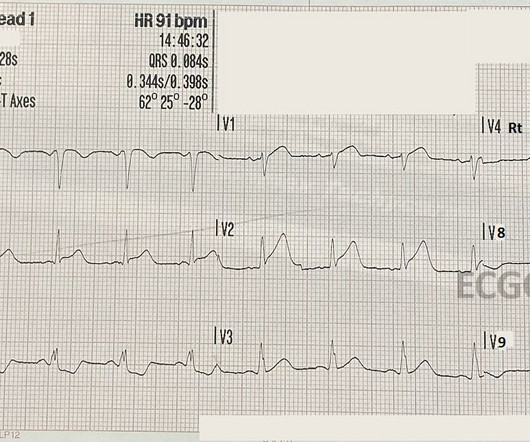
Of course he said: "Yes, it was a 60 year old diabetic with Chestpain." K en G rauer gives a thorough explanation here: A 60 year old with chestpain == MY Comment , by K EN G RAUER, MD ( 9/15 /2023 ): == The 1st time that I saw APTA ( A rterial P ulse T ap A rtifact ) — I did not know what it was. He said: "What?
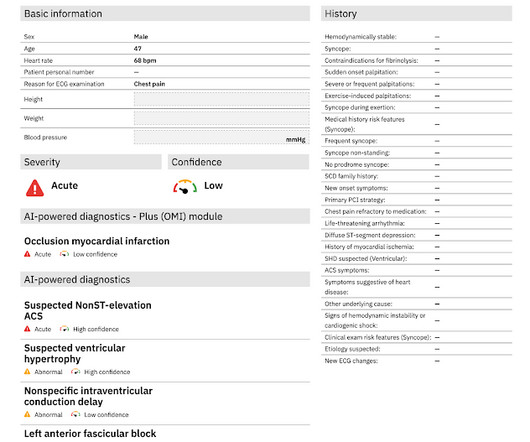
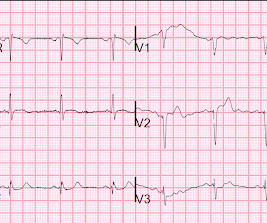
Written by Pendell Meyers Two patients with acute chestpain. Patient 1: Patient 2: Patient 1: A man in his 40s with minimal medical history presented with acute chestpain radiating to his R shoulder. Two patients with chestpain. Do either, neither, or both have OMI and need reperfusion?
Written by Pendell Meyers A man in his 40s called EMS for acute chestpain that awoke him from sleep, along with nausea and shortness of breath. His history included known heart failure with prior EF 18%, insulin dependent diabetes, and polysubstance abuse. Vitals were within normal limits except for tachypnea.
This results in severe chestpain or discomfort, with the subsequent release of cardiac biomarkers, and alterations in the electrocardiogram. Hypertension and diabetes were the two most common risk factors identified. It can cause diminished heart function and mortality if not treated properly with suitable measures.
Signs include: Sudden loss of consciousness No pulse or breathing Collapse without prior chestpain or discomfort If someone experiences sudden cardiac arrest, it is crucial to begin CPR immediately and call the local emergency number.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Past medical history included diabetes and hypertension.
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chestpain. As per Dr. Smith — today's patient is a 40-something year old patient with severe diabetes, renal failure and known coronary disease — who presents with “acute crushing CP”.
He had had several episodes of pain since onset; it was described as pressure-like and lasts about 5-15 minutes and resolves spontaneously. He had been pain free for about an hour. He had some "pre-diabetes ," but no h/o hypertension, no known family history of heart disease, and he smokes about 1-2 cigarettes per day.
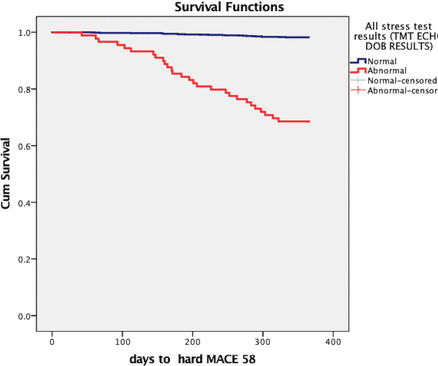
ObjectiveAlthough the association between admission glucose (AG) and major adverse cardiac events (MACE) is well-documented, its relationship with 30-day MACE in patients presenting with cardiac chestpain remains unclarified. years, with 1,028 (60.29%) being male and 500 (29.33%) having diabetes. The median AG levels were 7.60 mmol/L
A patient in their 40s with type 1 diabetes mellitus and hyperlipidemia presented to the emergency department with 5 days of “flu-like” illness. They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They denied fever, cough, dyspnea, and sick contacts.
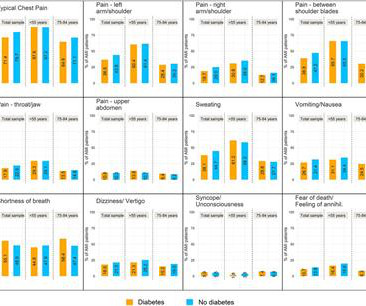
Background The objective of this study was to investigate the differences in presenting symptoms between patients with and without diabetes being diagnosed with an acute myocardial infarction (AMI). Results Patients with diabetes had significantly less frequent typical pain symptoms, including typical chestpain.
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. Without them the diagnosis is often tough and one must often rely on other clinical data- serial ECG’s, troponin, on-going chestpain, etc. This is particularly true in women, diabetics, and the elderly.
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He had history of prior MIs and CABG, as well as diabetes, hypertension, and hyperlipidemia.
Written by Jesse McLaren, with edits from Smith A 30 year old with a history of diabetes presented with two days of intermittent chestpain and diaphoresis, which recurred two hours prior to presentation. The chestpain was refractory to nitro so the cath lab was activated: 100% proximal LAD and 99% mid circumflex occlusions.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
While I still had questions about this case given the limited information provided ( ie, Was chestpain in this younger adult diabetic from acute PE? Was the ECG ever repeated?
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. Take home 1.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Sent by Pete McKenna M.D. Triage ECG: What do you think? This is diagnostic of proximal LAD occlusion. I cannot be anything else.
A 55 years old diabetic male patient who had 12 stents in his heart underwent a successful beating heart bypass surgery under Dr. Prateek Bhatnagar, Director Cardiac Surgery. The patient was suffering with angina (chestpain) since 2002. He was now getting chestpain even at rest and his life was at grave risk.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. <0.049 ng/mL).
Because previous ischemia induces myocardial preconditioning, decreasing the likelihood of transmural myocardial necrosis and myocardial rupture, patients with evidence of diabetes mellitus, chronic angina or previous MI are less likely to experience a rupture. Not all patients with acute ( or recent ) MI have chestpain with their event.
Introduction:Over 6 million patients (pts) present to US emergency departments annually with chestpain (CP), of which the majority are found to have no serious disease. Evaluation of these pts results in substantial costs for unnecessary hospitalization and extensive testing. Length of stay (LOS) in the CPU to discharge was 10.4
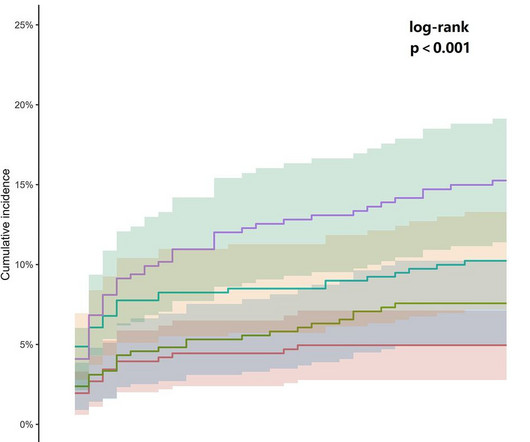
Multivariable Cox models, adjusted for clinical and imaging variables, showed that diabetes (HR: 2.38; p=0.008), HEART score of 3 (HR: 1.32; p=0.01), history of coronary artery disease (HR: 2.75; p=0.003), ECG changes (HR: 5.11; p<0.0001) and abnormal NISI (HR: 16.4;
Haechan Cho, MD received Best Abstract first runner-up after presenting his abstract, “Coronary Computed Tomography Angiography Versus Functional Testing In Patients With Diabetes And Suspected Coronary Artery Disease: Real-world Evidence From The Nationwide Cohort.”
This ECG was texted to me with the message "A 31 year old with Diabetes and HTN complains of bilateral arm tingling and headache." If it was chestpain it would be more difficult to go with my gut on that." Never chestpain but had to treat as hypertensive emergency. There is also STE in V2. What do you think?
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast.
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain.
In this case the diagnosis was easy because the patient presented very ill with known Type I diabetes and with vomiting, not chestpain. However, here are two from my files that presented with chestpain: The peaked T-waves give it away, but the ST elevation in V1 and V2 is a little known pseudoinfarction pattern.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
We found that a history of hypertension and diabetes are independent determinants of having a high-risk CAC score. There were 127 patients (11.2%) classified as high risk (CAC ≥400). Furthermore, this study demonstrated protective effects associated with physical activity and diastolic blood pressure.
The Patient: This series of ECGs is from a 65-year-old woman who was complaining of a sudden onset of chestpain, nausea, and weakness. She stated that the pain increased on inspiration. She reported a history of non-insulin-dependent diabetes mellitus (NIDDM). In chestpain, possible M.I.,
Patients with coronary artery diseaseplaque buildup inside the arteries that leads to chestpain, shortness of breath, and heart attackoften undergo PCI, a non-surgical procedure in which interventional cardiologists use a catheter to place stents in the blocked coronary arteries to restore blood flow.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Thanks for reading Dr. The data is overwhelming every way you can possibly look at it.
A 65 year old with diabetes presented with a syncopal episode while sitting, associated with weakness but no chestpain or shortness of breath. S yncope is an uncommon presentation of ACS, but anginal equivalents are more likely in older patients with diabetes 2. PEARL #1: Not all patients with acute MI report chestpain.
This was sent to me by a French colleague, Olivier Peyronie "Yesterday we received a 62 yo man with diabetes, hypertension and smoker. He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. You must record frequent serial ECGs for patients with chestpain.
Monitor cholesterol levels and manage conditions like diabetes that can strain the heart. Exercise regularly to keep the heart strong and healthy. Avoid excessive alcohol and drug use. See a doctor regularly to detect and treat any early signs of heart disease.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The syncope lasted about 2-3 minutes according to his wife.
Chestpain and discomfort, shortness of breath, exhaustion, lightheadedness, vertigo, ankle or leg oedema, and irregular pulse are some early warning signs of heart disease that are frequently experienced. Headaches Headaches might signify heart disease when accompanied by additional symptoms like shortness of breath or chestpain.
Most cases go undiagnosed until the condition advances enough to create symptoms such as shortness of breath, chestpain or fatigue. Valvular heart disease, a condition in which any of the heart’s four valves are damaged or diseased, afflicts 2.5 percent of all Americans and 13 percent of Americans over age 80.
Written by Pendell Meyers A male in his 50s with history of HTN, DM, HLD presented with chestpain of less than one hour duration. Here is a repeat ECG 45 minutes later with persistent chestpain: Obviously progressing into a clear STEMI. Here is his triage ECG: What do you think? The ECG was interpreted as non-ischemic.
Written by Pendell Meyers A woman in her 70s with diabetes, hypertension, and hyperlipidemia suddenly developed nausea, diaphoresis, and brief syncope while eating at a restaurant. She did not report any chestpain or pressure. A male in his 60s with chestpain A Male in his 60s with Chestpain.
This 57 yo diabetic male presented with generalized fatigue, myalgias, and arthralgias , mild subjective fever and chills, and nausea. He also stated his arms and head feel "heavy" and he had a headache, dry heaves, and dizziness, and some "indigestion" in his chest "like acid". He had been awakened by cough at 3 AM 2 days earlier.
female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chestpain for the past four hours. While she was in her bed at home, she had sudden onset of left sided chestpain that radiated to her shoulder. The pain was pleuritic, without nausea or diaphoresis.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content