This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male had onset of chestpain 1 hour prior to ED arrival. Endorses some associated SOB, but denies back pain, fever, cough, chills, leg swelling, or other new symptoms. It was tested on a large database of known outcomes and was more than twice as senstivity as STEMI criteria and much better than cardiologists.
I was working at triage when the medics brought this patient who is 65 yo and has had chestpain for 12 hours. I took the patient to the criticalcare area and questioned him more on the way. The pain had been intermittent until an hour before arrival, when he called 911. So I uncrumpled it: What do you think?
This 54 year old patient with a history of kidney transplant with poor transplant function had been vomiting all day when at 10 PM he developed severe substernal crushing chestpain. At first glance, it seems the patient is having a STEMI. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock.
This EKG was recorded as part of a standing order for criticalcare. Upon questioning patient, he denies having any chestpain or chest tightness of any sort. In the absence of chestpain and negative troponin , it appears less likely that he is having acute coronary syndrome though EKG appears concerning.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Is it normal STE?
He was a 30-something with chestpain. Prehospital ECG: Obvious anterolateral STEMI (Proximal LAD occlusion) The cath lab was activated prehospital by the medics. A male in his 30's complained of sudden severe substernal chestpain. Interventionalist at the Receiving Hospital: "No STEMI, no cath.
If you saw this ECG only knowing that it is an acute chestpain patient, what would be your interpretation? There was high suspicion of OMI, so patient was brought to criticalcare area and another ECG was recorded just 7 minutes later as the pain had diminished to 4/10. Suspicious but not diagnostic.
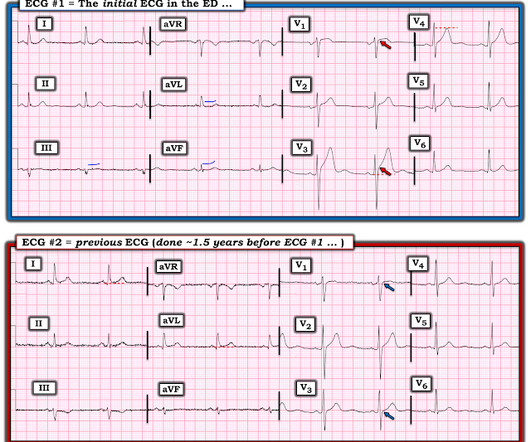
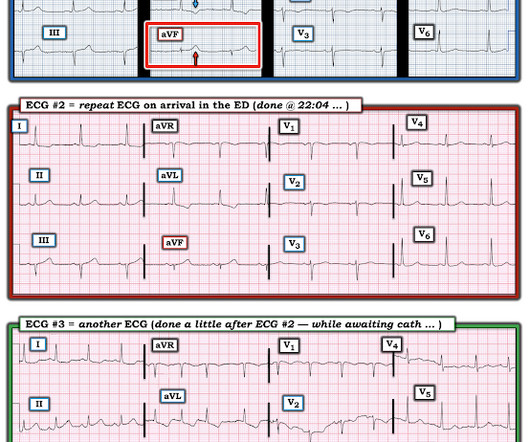
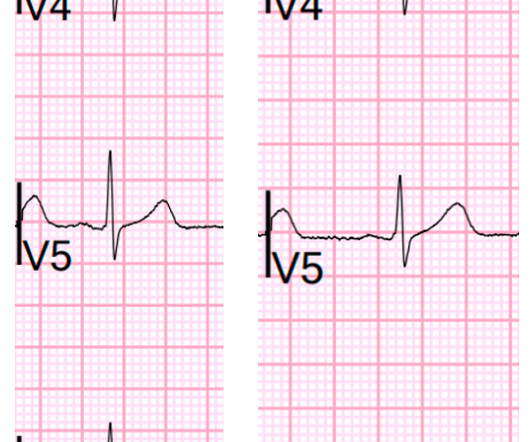
We knew only that the ECG belonged to a man in his 50s with chestpain and normal vitals. We brought the patient into one of our criticalcare rooms and immediately got more history while recording this repeat ECG: The STE in I has greatly diminished or entirely disappeared. No prior available. We activated the cath lab.
Submitted and written by Alex Bracey, with edits by Pendell Meyers and Steve Smith: I was walking through the criticalcare section of the ED when I overheard a discussion about the following ECG. The patient was given fentanyl initially for chestpain with minimal effect and then vomited which was followed by zofran and famotidine.
The patient was otherwise healthy, had no past history, and had never had chest discomfort before. I immediately activated the criticalcare team and walked the patient to the criticalcare area, our "Stabilization Room." This is why it is essential that the OMI/NOMI paradigm replace the STEMI/NonSTEMI paradigm.
Instead, he complained of left chest "itchiness". He was brought to the criticalcare area where these rhythms were seen on the monitor: Wide complex tachycardia with no apparent P-waves, and very irregular Consistent with atrial fibrillation with aberrancy A Regular wide complex tachycardia. LV Aneurysm?
This was sent by anonymous The patient is a 55-year-old male who presented to the emergency department after approximately 3 to 4 days of intermittent central boring chestpain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
A late middle-aged man presented with one hour of chestpain. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 Crit Care Med. Most recent echo showed EF of 60%.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. What is it?
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chestpain, dyspnea and weakness on the treadmill. In the ED he had some continued chestpain and hypotension. There is no acute STEMI. This is diagnostic of recent, reperfused STEMI. Plummer D et al.
Case 1: 20-something woman with chestpain Case 2: 50-something man with chestpain Case 1 A 20-something yo woman presented in the middle of the night with severe crushing chestpain. The blood pressure was 170/100 in the criticalcare area. No ECG was recorded after pain resolution.
Dizziness is so unlikely to be OMI without an obvious ECG, that I am going to pretend that this patient presented with chestpain. The PMCardio Queen of Hearts app asks you, before giving an interpretation of OMI ("STEMI-Equivalent"), whether the patient's clinical presentation is high risk for OMI. What do you think?
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. There is STE in V5-6. There are new Q-waves in aVL, V5-6. How do I know?
Just a few weeks ago, I took care of a patient who had ostial RCA OMI (TIMI 0 at cath) and his only complaint was syncope! He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. Multidisciplinary criticalcare management of electrical storm. link] Jentzer, J. Kashou, A.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content