This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Together, the two companies will work to further the development and commercialization of Medis Quantitative Flow Ratio (Medis QFR), a non-invasive approach to the assessment of coronary physiology, as part of GE HealthCare’s interventional cardiology portfolio built around the Allia Platform.
1 Atherosclerosis is a systemic disease that affects multiple vascular regions and is particularly severe in PAD patients, where up to 80 percent suffer from concurrent coronaryarterydisease (CAD), historically linked with a mortality rate exceeding 50 percent within five years. Journal of Vascular Surgery, Mar.
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, today announced the primary endpoint results of the open label roll-in cohort of the CardiAMP Cell Therapy in Chronic Myocardial Ischemia Trial. million patients in the United States.
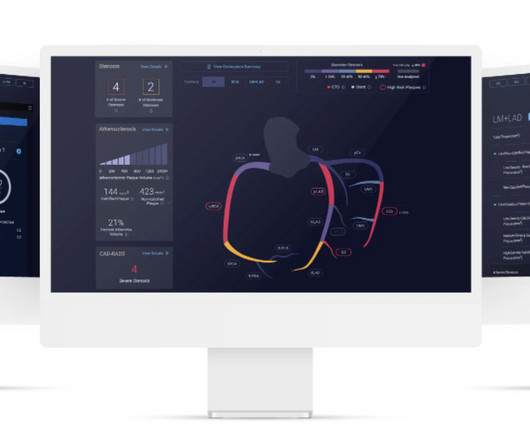
milla1cf Thu, 03/28/2024 - 07:00 March 28, 2024 — Cleerly , the company on a mission to create a new standard of care to aid in the diagnosis of heart disease, shared findings from a study published online in the Journal of the American College of Cardiology: Cardiovascular Imaging on March 13, 2024. JACC Cardiovasc Imaging. 2024.01.007.
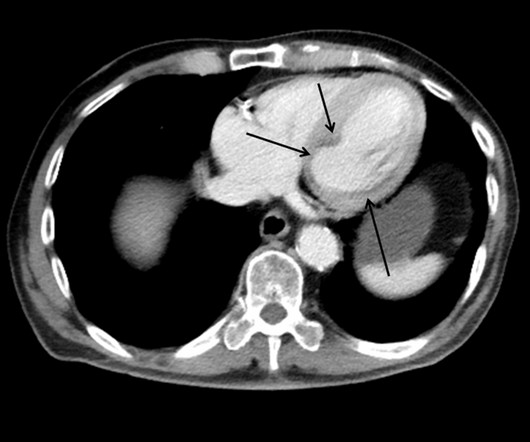
This case shows a CT image of subendocardial ischemia. This patient presented with a mechanical fall and had chestpain. His chestpain increased and this ECG was recorded: Now there is increasing inferior ST elevation. Severe Left Main disease, and chestpain with contrast injection into the LM.
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. More detailed reviews of subendocardial ischemia, as well as acute ECG patterns that breach the typical presentation, can be found here: [link] [link] Imaging revealed no acute head, or spinal, injuries.
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest. They agreed ischemia was likely in the setting of demand given DKA and infection.
ObjectiveA significant proportion (85%) of low-risk non-ST-elevation acute coronary syndrome (NSTE-ACS) patients do not receive objective confirmation of ischemia by stress echocardiography (SE), yet remain a healthcare burden due to lower long-term survival and overuse of medical services.
PCI is commonly used to open blocked arteries to treat significant myocardial ischemia , which occurs when the heart muscle does not get enough oxygenated blood. To test this strategy, researchers enrolled 1,606 patients treated for coronaryarterydisease at 15 centers in four countries.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Traditional methods of non-invasive ischemia testing (stress EKG , stress echo, SPECT , PET , direct-to-cath) can result in false negatives 20-30 percent of the time, which can lead to undetected disease, and false positives over 50 percent of the time, which can lead to unnecessary invasive procedures. Arbab-Zadeh, Heart Int 2012.
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronaryarterydisease and myocardial infarctions. On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. She's had multiple PCI procedures.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. His wife contacted the ambulance service after the patient experienced an episode of loss of consciousness.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronaryarterydisease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast.
Knowledge of this fundamental pillar of biology should drive how cardiologists approach men and women being evaluated for the presence of significant coronarydisease. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms. versus 66.3%; P =0.004), older age (62.4±7.9
Heart Valve Disease If one or more heart valves are not functioning correctly, it can cause blood to flow backward, putting extra pressure on the heart, which may cause it to expand to compensate for the inefficiency. This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge.
CT coronary angiography, in addition to a CT CAC, is arguably the best test for estimating whether someone has evidence of coronaryarterydisease and what that means for their near-term risk of a heart attack. This article is part 2 of a series on cardiac CT. I would say yes. For very good reason. And it matters.
In general, there is no debate here regarding the need for stenting a coronaryartery. Share Stenting In Stable CoronaryArteryDisease The real debate relates to the role of stenting in the setting of a severely narrow coronaryartery outside the setting of a heart attack. Makes total sense.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The diagnostic coronary angiogram identified only minimal coronaryarterydisease, but there was a severely calcified, ‘immobile’ aortic valve.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. There is no definite evidence of acute ischemia. (ie, The below ECG was recorded.
For example, if a coronaryartery becomes blocked due to plaque buildup (a condition known as coronaryarterydisease), the heart muscle may not receive enough oxygen, leading to chestpain (angina) or, in more severe cases, a heart attack. CAD is one of the leading causes of heart attacks.
CTA head and neck were obtained and showed no evidence of intracranial hemorrhage, large vessel occlusion stroke (what a helpful and apt name for an acute arterial occlusion paradigm, by the way.), or basilar ischemia. Preliminary findings documented in the cath lab were “Anterior STEMI and no significant coronaryarterydisease.” (!!!)
If you experience any symptoms, such as chestpain, dizziness, unusual tiredness or fatigue, shortness of breath, or irregular heartbeat, your doctor would want you to go for an ECG test to find out the underlying cause. An ECG or EKG monitor is used to detect diseases related to the heart.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Incidence of an acute coronary occlusion.
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. Back to the case: The providers recognized persistent ischemia and likely occlusion, and discussed this with cardiology who took the patient immediately for cath. They opened it.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Subscribe now Stenting stable coronaryarterydisease has not been convincingly proven to reduce the risk of future heart attacks or death 1. Whether stenting a narrowed coronaryartery improves symptoms such as chestpain (angina) or shortness of breath is a very different question. N Engl J Med.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronaryarterydisease? Ischemia b. ST depression: is it ischemia? It was a baseline finding in 62% of patients, usually due to LVH. Reference: Knotts RJ , Wilson JM, Kim E, Huang HD, Birnbaum Y.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronaryartery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Here I explain: First, you don't know for certain what the state of the artery was at the time of the ECG.
We knew only that the ECG belonged to a man in his 50s with chestpain and normal vitals. The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronaryarterydisease. He had no further pain and went to bed that night with no complaints.
A recent similar case: A 40-something with chestpain. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Acute ischemia? Is this inferior MI? Just as interesting is EKG 1, 24 minutes before the first: What do you think here?
Yang is also winner of the SCCT Best Abstract Award for his submission, “Coronary CT Angiography-derived Precursors Of Acute Coronary Syndrome In Ischemia-causing Lesions.” The SCCT Best Abstract Award is supported by the Cardiovascular Research Foundation of Southern California (CVRF of So.
In a study published by the American Heart Association, “Sex and Age Differences in the Association of Depression With Obstructive CoronaryArteryDisease and Adverse Cardiovascular Events,” researchers investigated 3,237 patients (35% women) undergoing coronary angiography to evaluate for coronaryarterydisease (CAD).
He has a history of coronaryarterydisease and a STEMI two years prior that was treated with primary PCI. He contacted EMS due to acute onset chestpain and feeling unwell and fatigued. He subsequently developed worsening chestpain. He was given ASA and sublingual NTG and taken to the ED.
Written by Pendell Meyers A woman in her 70s with known prior coronaryarterydisease experienced acute chestpain and shortness of breath. The chestpain was described as severe pressure radiating to both shoulders. Here is her ECG within 30 minutes of PCI: Improved, but still with ischemia.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronaryarterydisease presented with chestpain. He said he had had three episodes of chestpain that day while urinating. No evidence for ischemia jumps out.
The patient received three nitroglycerin tablets with significant "improvement" in his chestpain. Improved chestpain is unresolved chestpain. Improved chestpain is unresolved chestpain. I am commonly told, and I commonly read in the chart that chestpain is resolved.
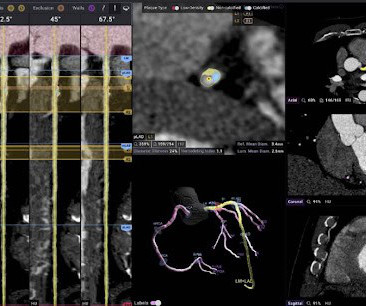
A recent study out of UCLA added to the growing body of evidence supporting AI-assisted CCTA as an alternative to SPECT for diagnosing obstructive coronaryarterydisease, especially in women. SPECT continues to be a first-line test to diagnose coronaryischemia, often instead of or before invasive coronary angiography.
BackgroundPainful left bundle branch block (LBBB) syndrome is an uncommon disease that is defined as intermittent episodes of angina associated with simultaneous LBBB changes on an electrocardiogram (ECG) with the absence of flow-limiting coronaryarterydisease or ischemia on functional testing.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
A 50-something man presented with worsening severe exertional chestpain which was just resolving as he had an ECG recorded in triage. Watch what happends as the heart recovers from its episode of ischemia. The ECG shows inferior ischemia. Are the T-waves in leads I and II hyperacute? Hard to tell. How can we know?
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. link] Myers, A., &
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content