This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This was sent by anonymous The patient is a 55-year-old male who presented to the emergency department after approximately 3 to 4 days of intermittent central boring chestpain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
High blood pressure, also known as hypertension, is a common condition that affects millions of people worldwide. Often referred to as the silent killer, hypertension can quietly damage your heart and other vital organs over time. Hypertension is diagnosed when blood pressure consistently reads 130/80 mm Hg or higher.
The National Institute for Health and Care Excellence (NICE) advise against routine testing for coronaryarterydisease (CAD) in patients with non-anginal chestpain (NACP). This analysis suggests age, male gender, Qrisk2 score and hypertension are predictors of CAD in this cohort.
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. Old ‘NSTEMI’ A history of coronaryarterydisease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis.
Non-ischemic phenotypes differed in the prevalence of hypertensive response, reduced CR, and reduced HRR. Among patients with non-ischemic phenotypes, the incidence of coronaryarterydisease was low (23%).ConclusionsFour
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Introduction:Over 6 million patients (pts) present to US emergency departments annually with chestpain (CP), of which the majority are found to have no serious disease. Evaluation of these pts results in substantial costs for unnecessary hospitalization and extensive testing. Length of stay (LOS) in the CPU to discharge was 10.4
There are numerous factors that can lead to cardiomegaly, ranging from temporary conditions to chronic diseases. High Blood Pressure (Hypertension) Persistent high blood pressure forces the heart to work harder to pump blood. Here are some of the most common causes: 1.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronaryarterydisease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast.
Knowledge of this fundamental pillar of biology should drive how cardiologists approach men and women being evaluated for the presence of significant coronarydisease. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms. versus 66.3%; P =0.004), older age (62.4±7.9
years]) admitted to the China ChestPain Center Database between 2016 and 2021. Hierarchical clustering of 15 medical conditions was performed to derive multimorbidity patterns. The primary outcome was a composite of inhospital adverse events.
Introduction:Since the advent of percutaneous coronary intervention (PCI), the scope of this therapeutic intervention has broadened to include cases of life-threatening multivessel coronaryarterydisease that previously may have only been corrected surgically.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The syncope lasted about 2-3 minutes according to his wife.
The complications of the procedure and patient’s outcomes were discussed.MethodsWe identified two patients who were admitted to our medical center between January 2022 to December 2022 for subclavian‐carotid artery bypass procedure. Clinical data were reviewed retrospectively.ResultsCase 1.
Family history – If a close family member has had heart disease, it can raise your risk. High blood pressure – Hypertension is a significant risk factor for heart disease. Heart issues can encompass a wide range of problems, from coronaryarterydisease to heart failure, arrhythmias and more.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. Takotsubo is a sudden event, not one with crescendo angina. Lindahl et al.
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. E CG # 1 was obtained in the referral hospital, approximately 2 hours after the onset of chestpain. This ECG was recorded on arrival: What do you think?
We knew only that the ECG belonged to a man in his 50s with chestpain and normal vitals. The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronaryarterydisease. He had no further pain and went to bed that night with no complaints.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting.
He has never had any chestpain. He has no known prior medical history and does not take any medications. He complains of occasional shortness of breath on walking more than 2 blocks. He has never smoked and denies any alcohol or drug abuse history. He was adopted and does not know anything about his parents or siblings.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronaryarterydisease? Does this patient have hypertension and/or heart failure that has worsened? This might be a common scenario given this patients demographics and his underlying disease ).
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The diagnostic coronary angiogram identified only minimal coronaryarterydisease, but there was a severely calcified, ‘immobile’ aortic valve.
Healy, MD, FACC, published an editorial in the New England Journal of Medicine highlighting the findings of two studies in that issue demonstrating clear evidence of sex bias in the management of coronaryarterydisease.2 That's the only way we can give women a definitive diagnosis for what's causing their chestpain."
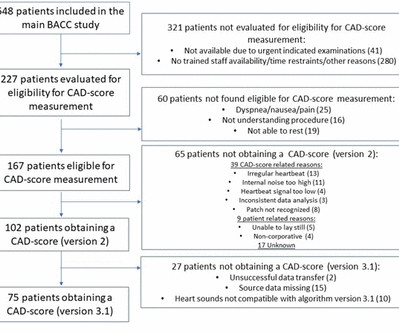
Background As only a small proportion of patients with chestpain suffers from myocardial infarction (MI), safe rule-out of MI is of immense importance. Recently an ultrasensitive microphone performing diastolic heart sound analysis (CADScorSystem) for rule-out of coronaryarterydisease (CAD) has emerged.
In a study published by the American Heart Association, “Sex and Age Differences in the Association of Depression With Obstructive CoronaryArteryDisease and Adverse Cardiovascular Events,” researchers investigated 3,237 patients (35% women) undergoing coronary angiography to evaluate for coronaryarterydisease (CAD).
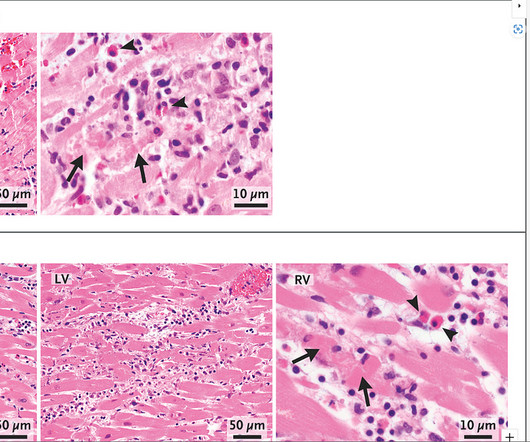
The case reports of vaccine myocarditis described to date describe a typical fulminant presentation of severe myocarditis: Sudden onset of shortness of breath or chestpain, followed by rapid clinical decompensation. One of the 2 cases described in the New England Journal of Medicine was diagnosed based on autopsy findings.
One of the most effective treatments for severe coronaryarterydisease, a type of cardiovascular disease, is coronaryartery bypass grafting (CABG), a procedure designed to restore blood flow to the heart. But does coronaryartery bypass surgery also improve erectile capacity?
Written by Willy Frick A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a risk factor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. Improved chestpain is unresolved chestpain. 50.000 ng/mL."
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content