This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The goal of the DISCHARGE trial was to evaluate computed tomography (CT) compared with invasive coronary angiography among patients with stable chestpain and intermediate pretest probability of obstructive coronaryarterydisease.
This prespecified secondary analysis of the Diagnostic Imaging Strategies for Patients With Stable ChestPain and Intermediate Risk of CoronaryArteryDisease (DISCHARGE) randomized clinical trial investigates the association of age with clinical outcomes after computed tomography and coronary angiography in stable chestpain.
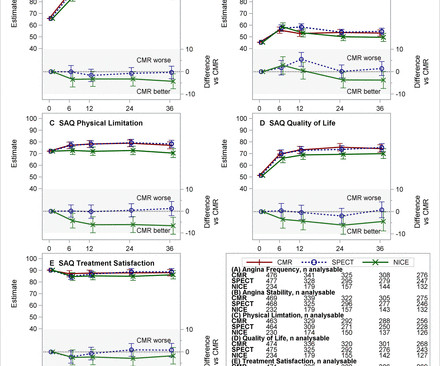
The National Institute for Health and Care Excellence (NICE) advise against routine testing for coronaryarterydisease (CAD) in patients with non-anginal chestpain (NACP). Over 23 months, 866 patients with NACP underwent CTCA.
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. Old ‘NSTEMI’ A history of coronaryarterydisease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis.
Previous studies have found less than 40% of patients with stable chestpain undergoing invasive coronary angiography are found to have obstructive coronaryarterydisease.
A healthy 45-year-old female presented with chestpain, with normal vitals. The patient was previously healthy, with no atherosclerotic risk factors, and developed chestpain after an episode of stress. The pain was crushing retrosternal, radiated to the arms and was associated with lightheadedness.
Aims Guidelines for suspected cardiac chestpain have used historical risk stratification tools, advocating invasive coronary angiography (ICA) first-line in those at highest risk.
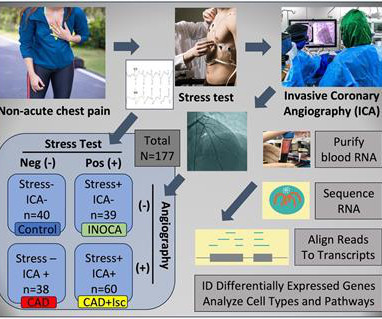
Background:Patients with de novo chestpain, referred for evaluation of possible coronaryarterydisease (CAD), frequently have an absence of CAD resulting in millions of tests not having any clinical impact. Circulation: Genomic and Precision Medicine, Volume 16, Issue 5 , Page 442-451, October 1, 2023.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. Cath lab activation by the ED and I agree with coronary angiography emergently." Result: no angiographically significant obstructive coronaryarterydisease. What do you think? Medical Rx.
This interest may be attributed in part to a 2021 decision by the American College of Cardiology (ACC) and the American Heart Association (AHA) to give cardiac CT angiography (CCTA) its highest recommendation as a frontline test to evaluate patients with stable and acute chestpain who have no history of coronaryarterydisease.¹
CoronaryArteryDisease (CAD) : High blood pressure accelerates the development of CAD by promoting the buildup of plaques in the coronaryarteries. This condition reduces blood flow to the heart, increasing the risk of angina (chestpain) and heart attacks.
Undergoing heart surgery can be a life-changing experience, especially for those with coronaryarterydisease or other heart conditions. Pay attention to how your body responds, particularly monitoring for chestpain or unusual shortness of breath.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Coronary computed tomography (CCTA), used for first-line investigation of chestpain, has revealed there is a large group of individuals without obstructive coronaryarterydisease (CAD) for whom there is an unclear prognosis and management.
With more than 500 peer-reviewed publications, the HeartFlow FFR CT Analysis remains unparalleled in precision coronary care, as supported by the ACC/AHA ChestPain Guidelines, to improve treatment plans and outcomes. 2021 ACC/AHA ChestPain Guidelines. For more information: www.heartflow.com References 1.
Among patients with non-ischemic phenotypes, the incidence of coronaryarterydisease was low (23%).ConclusionsFour Non-ischemic phenotypes differed in the prevalence of hypertensive response, reduced CR, and reduced HRR.
Haechan Cho, MD received Best Abstract first runner-up after presenting his abstract, “Coronary Computed Tomography Angiography Versus Functional Testing In Patients With Diabetes And Suspected CoronaryArteryDisease: Real-world Evidence From The Nationwide Cohort.”
BackgroundVasospastic angina usually presents with intermittent episodes of chestpain. It can rarely be associated with the perception of phantom odors.Case summaryA 69-year-old woman presented for evaluation of intermittent shortness of breath and chestpain.
The patient’s chestpain (CP) was not alleviated with initial revascularization of his left circumflex (LCx) ST, requiring PCI to his right coronaryartery (RCA) chronic total occlusion (CTO).
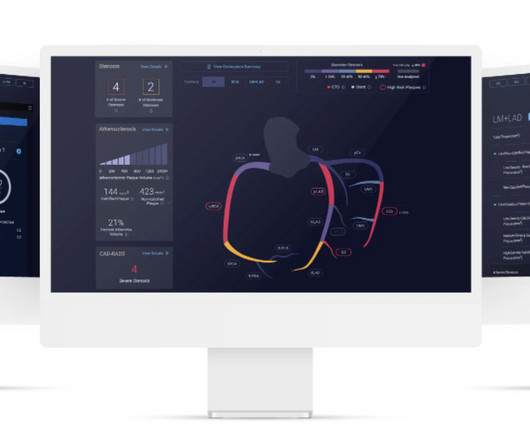
"This pivotal study was performed in two different international populations which shows that CCTA analyzed with the Cleerly AI-QCT ISCHEMIA device provides an accurate assessment of coronary ischemia,” said James P. Earls, MD , Chief Medical Officer of Cleerly. JACC Cardiovasc Imaging. 2024 Feb 29:S1936-878X(24)00039-1. doi: 10.1016/j.jcmg.2024.01.007.
A 30-something male presented in the middle of the night with several hours of sharp, non-radiating, left sided chestpain. No angiographically significant obstructive coronaryarterydisease. It was there earlier, went away, and then returned approximately 1 hour prior to arrival. Exam and vital signs were normal.
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest. He was treated for infection and DKA and admission to hospital was planned.
An 80-year-old man with renal disease on hemodialysis, coronaryarterydisease, complete heart block and a dual chamber leadless pacemaker (LP) implanted because of previous bacteremia, presented with syncope. An echocardiogram showed newly reduced left ventricular ejection fraction of 30-35%.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronaryarterydisease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast.
BackgroundIschemia with non-obstructive coronaryarteries (INOCA) is a major clinical entity that involves potentially 20%–30% of patients with chestpain. INOCA is typically attributed either to coronary microvascular disease and/or vasospasm, but is likely distinct from classical coronaryarterydisease (CAD).ObjectivesTo
Objectives There are few reports regarding the prognosis in patients with obstructive coronaryarterydisease (OCAD) and vasospastic angina (VSA). An obstructed coronaryartery was defined as ≥50% luminal narrowing.
Objective Cardiac cephalalgia, once seen as a rare symptom of coronaryarterydisease, is now more recognized. It often comes with chest discomfort and autonomic dysfunction, worsened by physical activity. However, not all cases have chest symptoms or are activity induced.
About Chronic Myocardial Ischemia with Refractory Angina Chronic myocardial ischemia occurs in the setting of coronaryarterydisease when there is reduced blood flow to the heart. million patients in the United States.
Introduction:Since the advent of percutaneous coronary intervention (PCI), the scope of this therapeutic intervention has broadened to include cases of life-threatening multivessel coronaryarterydisease that previously may have only been corrected surgically.
Heart bypass surgery, or coronaryartery bypass graft surgery (CABG), is performed to treat patients with severe coronaryarterydisease (CAD). As a result, the heart doesnt receive enough oxygen-rich blood, which can lead to chestpain, shortness of breath, or even a heart attack.
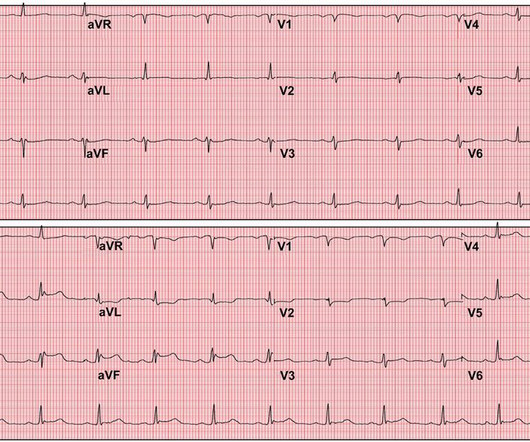
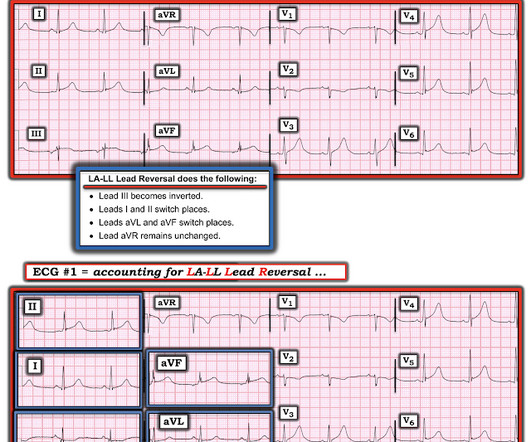
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. There is increased LV cavity dimensions with an increase in transient ischemic dilation, suggesting Left Main, or 3-vessel coronaryarterydisease. The fall was not a mechanical etiology.
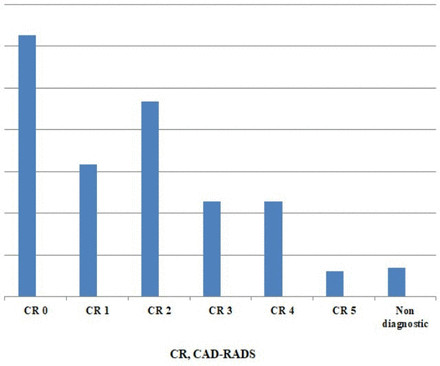
Uniform reporting was agreed including indication, BB administration, demographics, dose length product (DLP) and the coronaryarterydisease—reporting and data system (CAD-RADS) score. Uncertain CAD-RADS meant a non-diagnostic scan (NDS).
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronaryarterydisease and myocardial infarctions. On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. She's had multiple PCI procedures.
years]) admitted to the China ChestPain Center Database between 2016 and 2021. Hierarchical clustering of 15 medical conditions was performed to derive multimorbidity patterns. The primary outcome was a composite of inhospital adverse events.
Assessment of patients presenting for the first time with suspected coronaryarterydisease (CAD) remains cumbersome with multiple diagnostic options. Likelihood of CAD can be estimated based on symptoms and risk factors, and an abnormal ECG may also be helpful.
Per the new LCDs, AI-CPA using coronary computed tomography angiography (CCTA) is considered reasonable and medically necessary as a diagnostic study when the patient is eligible for CCTA; and the patient presents with acute or stable chestpain and is at intermediate risk for coronaryarterydisease (CAD) or has evidence of CAD-RADS™ level 1, 2 or (..)
63 years old Afsar Khan resident of Karwan, Hyderabad had been having coronaryarterydisease and chestpain on exertion for about a year. In November 2019, he underwent CT coronary angiography which showed blocks in all 3 coronaryarteries of the heart. He was still corona negative.
a med tech company dedicated to helping patients with persistent ischemic heart disease, has announced the treatment of the first patient with the A-FLUX Reducer System, a treatment for patients with angina or chestpain. VahatiCor, Inc., Angina is often caused by reduced blood flow to the heart.
Patient Mr. Paras Ram was having unstable angina (chestpain at rest) at his native place. Coronary angiography showed tight left main coronaryarterydisease with severe triple vessel disease. All his coronaryarteries were heavily calcified.
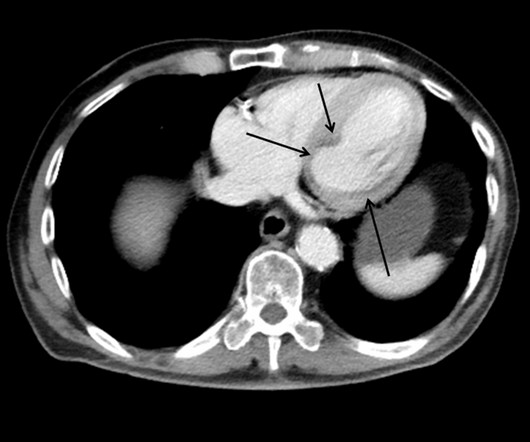
This patient presented with a mechanical fall and had chestpain. His chestpain increased and this ECG was recorded: Now there is increasing inferior ST elevation. Severe Left Main disease, and chestpain with contrast injection into the LM. This case shows a CT image of subendocardial ischemia.
Here is the clinical story: A 40 year old male with no cardiac history presented with acute substernal chestpain that started 40 minutes prior to arrival. In spite of a relatively short QTc of 376 ms, the very low R-wave amplitude in V4 and the ST Elevation at 60 ms after the J-point in lead V3 contribute to a high final value.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content