This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
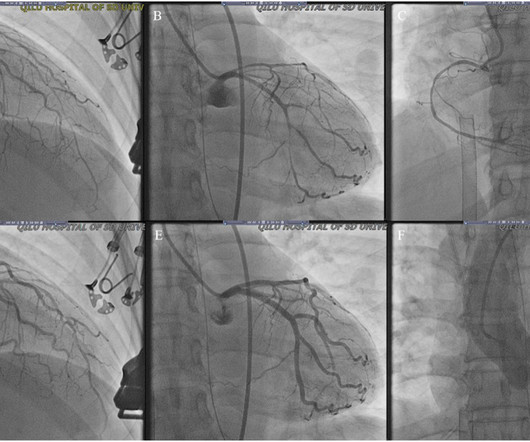
CT Coronary Artery Calcium Score Scan CT Coronary Artery Calcium Score CT CoronaryAngiogram As you can see from the above images, the CTCA provides far more anatomical detail. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test.
They knew they had not been doing all the things they should do, and they were worried that heartdisease had them in its sights. Risk factors such as high blood pressure, smoking, and inactivity are important because the longer you are exposed to them, the higher the odds you will develop coronary artery disease sooner in life.
Knowledge of this fundamental pillar of biology should drive how cardiologists approach men and women being evaluated for the presence of significant coronarydisease. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms.
He had concurrent sharp substernal chestpain that resolved, but palpitations continued. Over past 3 months, he has had similar intermittent episodes of sharp chestpain while running, but none at rest. Past medical history includes coronary stenting 17 years prior.
He has never had any chestpain. He has no known prior medical history and does not take any medications. He complains of occasional shortness of breath on walking more than 2 blocks. He has never smoked and denies any alcohol or drug abuse history. He was adopted and does not know anything about his parents or siblings.
He denied chestpain or dyspnea throughout. Discussion Thus, no further ECGs were recorded and there was no angiogram or stress test or CT coronaryangiogram. No previous study for comparison. Clinical Course: - He had no events on cardiac monitoring overnight. -
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The diagnostic coronaryangiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve.
The left and right coronary arteries were slender and narrow, which was relieved after the injection of 100g nitroglycerine through the left coronary artery. After performing a coronaryangiogram, the patient was given long-acting nitrates and calcium channel blockers orally, and her chestpain did not reoccur.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content