This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
They shocked him twice before return of spontaneous circulation. Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. He did not remember whether he had experienced any chestpain. When EMS arrived the patient was in ventricular fibrillation.
Written by Jesse McLaren A previously healthy 50 year-old presented with 24 hours of intermittent exertional chestpain, radiating to the arms and associated with shortness of breath. In a previously healthy patient with new and ongoing chestpain, this is concerning for acute occlusion of the first diagonal artery.
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. EMS recorded the following ECG: What do you see? The computer read "Right Bundle Branch Block" There is RBBB and LAFB, which can make it difficult to see the end of the QRS.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. It was not relieved by anything. He had no previous medical history.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, Pericarditis would be even more unlikely in someone without chestpain.
Circulation, Volume 150, Issue Suppl_1 , Page A4137144-A4137144, November 12, 2024. Introduction:Subacute stent thrombosis (ST) is related to high rates of cardiac reinfarction. He had CCS Class IV CP despite medical therapy and returned for re-look CA with TIMI-3 flow in the left-sided circulation without thrombus (Fig 1b).
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. Circulation 2014 2. The patient was transferred to CCU to consider surgical options. link] References 1.
See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. This is different from nitroglycerin which produces vasodilation and can improve by pain improving myocardial perfusion. Here is the angiogram after stent placement. Circulation , 130 (25). See this case: A man his 50s with chestpain.
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chestpain and collapsed, and had bystander CPR. On arrival, GCS was 13 and the patient complained of ongoing chestpain. So the RCA was stented.
He had no previous history of CAD, and presented with very typical waxing and waning chestpain, much worse with exertion but also present at rest and on presentation, though his pain was minimal at the time of the ECG. Two stents were placed. I saw this 59 year old male 3 weeks ago. Blood pressure was 150/80.
This 42 yo diabetic male presented with cough and foot pain. In spite of aggressive questioning, he denied chestpain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4.
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. A stent was placed. Type B waves are deeper and symmetric.
Circulation, Volume 150, Issue Suppl_1 , Page A4145631-A4145631, November 12, 2024. This was treated with a drug-eluting stent, but TIMI 3 flow was not achieved. Urgent angiography revealed complete occlusion with thrombus of the proximal left anterior descending (LAD) coronary artery.
Circulation, Volume 150, Issue Suppl_1 , Page A4139995-A4139995, November 12, 2024. Patients without data on C-reactive protein and high-density lipoprotein cholesterol and those who had a history of coronary artery bypass grafting and stenting in the left anterior descending artery were excluded. Recently, Rinaldi et al.
Pain worsened and became sharper after lifting a bookcase up the stairs. He continued to have worsening pain and diaphoresis, and associated left arm pain down to the fingers. reports MI in 2001 with a stent placed in the "marginal" artery. Pain is similar, but associated with less SOB. Exam is unremarkable.
It means either a percutaneous coronary intervention with a stent or CABG. You may be. But I am not.You need to undergo some re-vascularisation procedure. What do you mean by that Doctor ? Can I get my heart re-vascularised by drugs alone Doctor ? No we can’t. Hmmm , wait, we do have something called OMT/GDMT.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
This can block smooth flow of blood and the person can develop chestpain. The surgery was mostly done using a bone splitter to open the breast bone and with heart lung machine to support circulation when the heart is stopped. But now beating heart bypass surgery is commonly done.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. It was stented.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. Case 3 : Male in 30's with chestpain, cough, and fever. A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. This is a very common misread. What do you think? Called 911.
60-something with h/o MI and stents presented with chestpain radiating to the back and nausea/vomiting. It was stented. The patient had a p rior h istory of MI + stents. Time zero What do you think? There is inferior ST elevation. Is it normal variant? Is it ischemic (OMI)? Pericarditis?
Troponin elevation is dependent on presence or absence of occlusion (remember many OMI receive a diagnosis of NSTEMI), duration of occlusion (which is dependent on rapidity of therapy or the luck of spontaneous reperfusion), area of myocardium at risk, collateral circulation, and more. The lesion was stented. Circulation.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chestpain for 1.5 It was treated with and dual "kissing balloons" and drug eluting stents. Circulation 1993; 88:896-904. Circulation 1995; 91:1659-1668. Circulation 1999; 74:1379-1389. Circulation 1990; 82:1147-1158.
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. Despite the clinical stability and decreasing pain, this patient needs an immediate angiogram. Circulation 2002; 105(4): 539-42.
Below are 6 anecdotal cases of true complete left main occlusion with no collateral circulation: 3 have STE in aVR 1 has no ST shift in aVR 2 have STD in aVR The ECG can have a variety of presentations in LM Occlusion. You'll see that there is collateral circulation from the RCA. This is her ECG: An obvious STEMI, but which artery?
Case submitted and written by Dr. Mazen El-Baba and Dr. Emily Austin, with edits from Jesse McLaren A 50 year-old patient presented to the Emergency Department with sudden onset chestpain that began 14-hours ago. The pain improved (6/10) but is persisting, which prompted him to visit the Emergency Department. What do you think?
A late middle-aged man presented with one hour of chestpain. This was stented. mEq of K pushed fast and circulated theoretically would raise serum K immediately by 1.0 Most recent echo showed EF of 60%. He also had a history of chronic kidney disease, stage III. He had recently had a NonSTEMI. The patient stabilized.
When a person experiences a heart attack or myocardial infarction, they may feel chestpain and other symptoms in different parts of their body. This indicates that restoring normal blood circulation as quickly as possible will result in less damage. So, how do you recognize a heart attack? Perform rescue breaths twice.
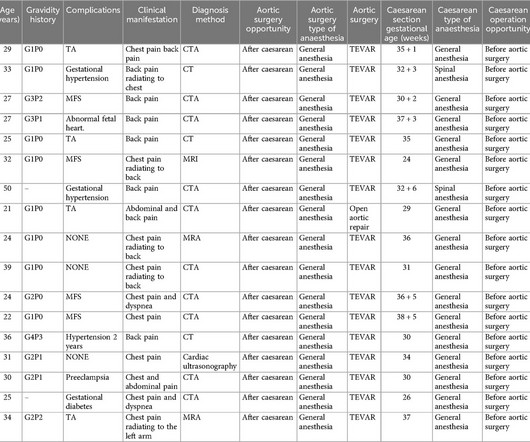
Type B aortic dissection (TBAD) during pregnancy is a rare disease, which is mostly caused by the increase of blood volume in circulation during pregnancy, the effect of estrogen and progesterone on the aorta, or congenital diseases. TBAD in TA pregnant women is very rare, and the condition is often complicated. She had TA for five years.
Written by Willy Frick A woman in her 60s with very severe hyperlipidemia (LDL >200 mg/dL) presented with acute onset chestpain. She described the pain as moderate in severity, and said it had come and gone several times over the next few hours before ultimately resolving. Her symptoms began while getting off the bus.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all. Circulation , 92 (3), 657671.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content