This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
25 in Chicago and simultaneously published in Circulation: CardiovascularImaging. 25 in Chicago and simultaneously published in Circulation: CardiovascularImaging.
Researchers have developed a new catheter-based device that combines two powerful optical techniques to image the dangerous plaques that can build up inside the arteries that supply blood to the heart.
The definition of a high-risk plaque should be expanded beyond the traditional focus on plaque rupture and thin-cap fibroatheroma in the setting of acute coronary syndromes (ACS), according to a new JACC: CardiovascularImaging Position Statement.
Circulation: CardiovascularImaging, Ahead of Print. BACKGROUND:Recently, it was reported that noncalcified plaque (NCP) volume was an independent predictor for cardiac events. P<0.001) than the group with low NCP plaque volume. P<0.001) than the group with low NCP plaque volume. versus 75.9%;P<0.001),
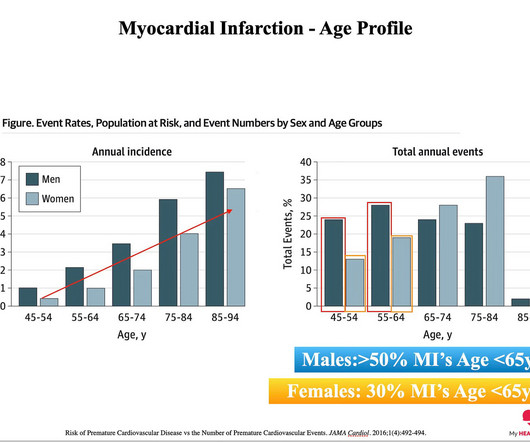
The reason: They were accumulating plaque in their coronary arteries much earlier than their peers. You can’t have a heart attack if you don’t have plaque in your coronary arteries. And plaque in your coronary arteries is the result of exposure to risk factors over time. The answer: Risk Factors. The answer.
Circulation: CardiovascularImaging, Ahead of Print. A decrease in the percentage of unstable core (fibro-fatty+necrotic plaque; from 14.1 [7.9–22.3] BACKGROUND:Intensive lipid-lowering therapy may induce coronary atherosclerosis regression. The global coronary PB changed from 34.6% (32.5%–36.8%) 36.8%) at entry to 30.4% (27.4%–33.4%)
Christian Tesche (Division of CardiovascularImaging, Department of Radiology and Radiological Science, Medical University of South Carolina and Department of Cardiology, Munich University Clinic, Ludwig-Maximilian-University).
25, 2024 in the European Heart Journal CardiovascularImaging. 25, 2024 in the European Heart Journal CardiovascularImaging 1. 25, 2024 in the European Heart Journal CardiovascularImaging 1. Presented at the European Association of CardiovascularImaging: Late Breaking Clinical Research and Trials.
Cardiovascular AI maintains a (distant) second largest share of FDA-cleared AI products, with 10% of total clearances (90), well below radiology’s 76% share (671). Cardiovascular AI actually makes up a larger 17.4% FFRCT, coronary plaque, etc). in 2020-2022, and 13.5% since the start of 2023.
in European Association of CardiovascularImaging: Late Breaking Clinical Research and Trials. With Plaque Features Associated with False Positives. Derivation, Validation and Prognostic Assessment of an AI-Based Algorithm for Determination of Coronary Ischemia: The CREDENCE and PACIFIC Trial. Barcelona, Spain.
However, cardiovascular AI actually made up a larger 18% share of total H1 2024 clearances (19 devices) if you also count cardiovascularimaging AI products that the FDA technically categorized within its “Radiology” segment (e.g.
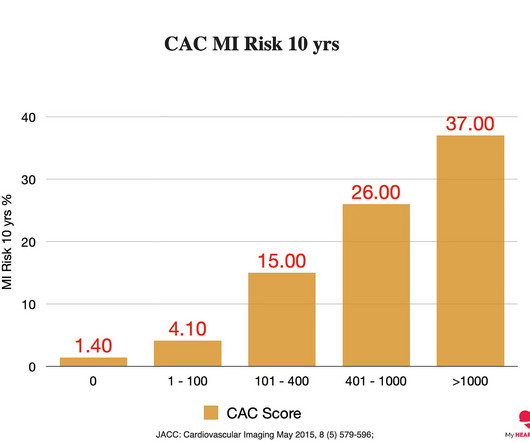
The most accurate way (But not the only way) to answer this question is whether or not you have plaque in your coronary arteries. If you already have plaque, your risk of event an event goes up proportional to the amount of plaque you have 2. 2 JACC: CardiovascularImaging May 2015, 8 (5) 579-596; 2022;18(6).
mg)has potential to directly reduce inflammation, which plays a substantial role in the formation and progression of atherosclerotic plaque leading to heart disease, said Matthew J. mg improved several measures of plaque volume changes over a period of 12 months in patients with stable coronary artery disease, Dr. Budoff continued.
This funding will allow us to expand our commercial reach, which is especially germane following our recent achievements in attaining Medicare coverage and a CPT Category I code for advanced plaque analysis. Barclay continued, “Cardiovascular disease is the #1 cause of death globally and costs our country $422B annually.
A cardiac CT is a low-dose CT scan of your heart that assesses whether or not you have plaque in your coronary arteries and, if so, how much. In general, the more plaque you have, the higher your risk of a heart attack over the next 10 years. 6, 2017 7 JACC: CardiovascularImaging May 2015, 8 (5) 579-596;
a leader in non-invasive artificial intelligence (AI) heart care solutions, announced that the data from its REVEALPLAQUE study , highlighting the accuracy of its Plaque Analysis, was published in the European Heart Journal CardiovascularImaging. milla1cf Thu, 05/23/2024 - 08:00 May 23, 2024 — HeartFlow, Inc. ,
Circulation: CardiovascularImaging, Volume 17, Issue 2 , Page e016178, February 1, 2024. BACKGROUND:It is not known whether there is a sex difference in the association between perivascular inflammation and plaque vulnerability. All images were analyzed at a core laboratory. plaques per patient). versus 46.9%,P=0.002
mg)has potential to directly reduce inflammation, which plays a substantial role in the formation and progression of atherosclerotic plaque leading to heart disease, said Matthew J. mg improved several measures of plaque volume changes over a period of 12 months in patients with stable coronary artery disease, Dr. Budoff continued.
Circulation: CardiovascularImaging, Ahead of Print. Coronary plaques were qualitatively classified as noncalcified or calcified plaques in each vessel. Hounsfield unit,P<0.01), as well as the presence of CCTA-defined mixed or noncalcified plaque anywhere in the coronary tree (65.5% versus 51.7%,P=0.01),
Baseline tissue characterisation includes the morphological description of culprit lesion plaque characteristics and thrombus as assessed with HD-IVUS. Study findings will be submitted to international peer-reviewed journals in the field of cardiovascularimaging and interventions and will be presented at international scientific meetings.
Therefore, if someone presents with an event earlier than this age, they likely have been building up plaque for a considerable period prior to this. A CT CAC score of 0 means a person has no calcified coronary artery plaque and also means their risk of a heart attack over the next ten years is probably less than 2%. Genes (Basel).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content