This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
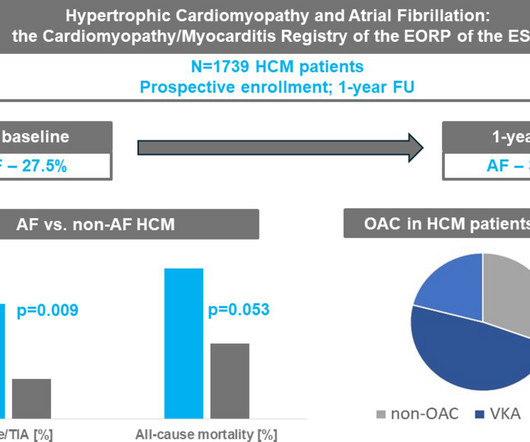
Background Hypertrophic cardiomyopathy (HCM) is commonly associated with atrial fibrillation (AF), but its impact on outcomes in real-world practice is uncertain. years) were enrolled in the EURObservational Research Programme (EORP) Cardiomyopathy/Myocarditis Registry. Methods Overall, 1739 adult patients with HCM (40.9%
Then I always look to see if the initial deflection of the QRS has a lot of voltage change per change in time (seen in tachycardias that are initiated from above the ventricle because the propagate through fast conducting purkinje fiber. Patient has an ICD, which is primarily placed in patients with cardiomyopathy.
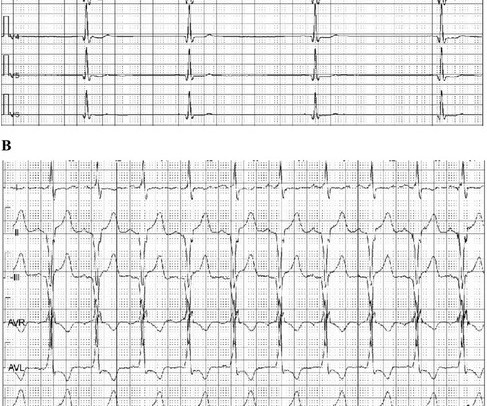
The ECG is from a 56-year-old man with severe ischemic cardiomyopathy who had an ICD implanted a few months ago due to recurrent ventricular tachycardia. Here we see a single-channel ECG, each line representing about 30 seconds. The explanation of what can be seen on this ECG can be found on the 2nd image.
BackgroundHypertrophic cardiomyopathy (HCM) is an autosomal dominant disorder characterized by asymmetric hypertrophy of the ventricles and the ventricular septum, leading to subsequent left ventricular outflow tract (LVOT) obstruction and diastolic dysfunction.
Among patients with ventricular tachycardia and ischemic cardiomyopathy, catheter ablation as an initial therapy led to a lower risk of adverse outcomes than antiarrhythmic drug therapy.
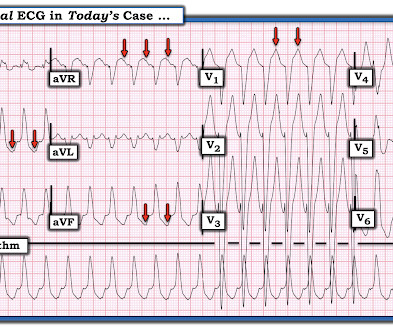
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Description : Regular Wide Complex Tachycardia at a rate of about 160. SVT with aberrancy?
And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis.
The goal of the VANISH2 trial was to compare endocardial catheter ablation with conventional antiarrhythmic drug (AAD) therapy as a first-line treatment for infarct-related ventricular tachycardia (VT) in ischemic cardiomyopathy.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
DCM had higher T1 and lower vGLNU than HC. When compared with TIC, DCM showed significantly higher LVEDV and LVEDVi. ROC analysis revealed that LVEDV and vGLNU provided high specificity for differentiating DCM from the other etiologies.ConclusionNative T1 mapping and its texture analysis may be valuable for differentiating between DCM and HC.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation.
The best approach for ablating ventricular tachycardia (VT) targeting right ventricular free wall (RVFW) aneurysms in arrhythmogenic right ventricular cardiomyopathy (ARVC) remains undefined.
Cardiomyopathy is a common underlying cause of ventricular tachycardia (VT). However, the differences in outcomes between patients with VT due to ischemic cardiomyopathy (ICM) and those with non-ischemic cardiomyopathy (NICM) remain unclear.
Tachycardia-induced cardiomyopathy (TIC) is a unique cardiomyopathy, which is potentially reversible. Due to the presence of tachyarrhythmias in various cardiomyopathies, differentiating TIC from other non-reversible conditions can be challenging.
Truncating variants in the TTN gene (TTNtv) are the most common cause of idiopathic/familial dilated cardiomyopathy (DCM) and are implicated in atrial fibrillation (AF).
Hypertrophic cardiomyopathy (HCM) patients undergoing ventricular tachycardia (VT) ablation face unique challenges due to underlying myocardial abnormalities. It is unclear how the presence of HCM affects outcomes of catheter ablation for VT.
The ECG in Figure-1 — was obtained from a middle-aged woman with positional tachycardia and diaphoresis with change of position from suprine to sitting. My THOUGHTS on the ECG in Figure-1: The rhythm is sinus tachycardia at ~105/minute ( ie, The R-R interval is regular — and just under 3 large boxes in duration ).
Tachycardia-induced cardiomyopathy refers to changes in cardiac structure and function that result from rapid arrhythmia and can manifest as a continuous or recurrent event. Cardiomyopathy induced by atrial ta.
Tachycardia-induced cardiomyopathy (TICM) is a reversible impairment of the left ventricular (LV) systolic function caused by persistent tachyarrhythmias. It is often difficult to identify macroscopic scar in patients with TICM by cardiac magnetic resonance imaging (MRI).
The ventricular tachycardia (VT) substrate in patients with non-ischemic cardiomyopathy (NICM) is complex in distribution and intramural location. Myocardial lipomatous metaplasia (LM) is vital to post-infarct VT circuitry, but not investigated in NICM VT circuitry yet.
Cardiac sarcoidosis (CS), a rare condition characterized by non-caseating granulomas, can manifest with symptoms such as atrioventricular block and ventricular tachycardia (VT), as well as mimic inherited cardiomyopathies. A 58-year-old woman presented with sustained VT with a prior diagnosis of hypertrophic cardiomyopathy (HCM).
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a family inherited cardiomyopathy associated with ventricular arrhythmias. With the development of molecular biology, histology, imaging, and other dia.
Chagasic cardiomyopathy has been associated with high defibrillator shock rates and poor clinical outcomes. The benefits of VT ablation in patients with Chagasic cardiomyopathy have been evaluated in only a few studies. Chagas disease is an endemic condition in Latin America.
Many genetic non-ischemic dilated cardiomyopathies (NICM) cause ventricular tachycardias (VT) originating from scar substrate identified as areas of low electrogram voltage. Substrate locations vary and the causes of scar are not well defined.
Catheter ablation is an effective tool to reduce ventricular tachycardia (VT) burden. There is a lack of robust data studying the intraprocedural characteristics and outcomes of VT ablation in patients with non-ischemic (NICM) versus ischemic cardiomyopathy (ICM).
Ventricular Tachycardia (VT) is an important cause of morbidity and mortality in structural heart Disease. Current literature is limited in direct comparison of VT in ischemic (ICM) compared to non-ischemic cardiomyopathy (NICM).
Catheter ablation (CA) is effective in the treatment of ventricular tachycardia (VT). Although some data suggest patients with non-ischemic cardiomyopathy (NCIM) have worse outcomes compared to those with an ischemic etiology (ICM), direct comparisons are scarcely reported.
Patients with non-ischemic left ventricular dilated cardiomyopathy (NIDCM) and ventricular tachycardia (VT) typically have a basal perivalvular substrate adjacent with specific distribution dependent on the genetic background.1-4 1-4 Isolated apical substrate responsible for VT in NIDCM with perivalvular sparing is rare.
Peri-Aortic ventricular tachycardia (peri-Ao VT) is frequently encountered in LMNA and TTN non-ischemic cardiomyopathy (NICM) and ablation outcomes remain suboptimal. The impact of the underlying genotype on VT ablation outcomes are largely unknown.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
A 69-year-old man with a history of MI and cardiomyopathy presented with 2 days of dyspnea. Regular tachycardia (124 beats per min), diaphoresis, and rales were present. A diagnosis was made.
He had a background of arrhythmic right ventricular cardiomyopathy. He had previously undergone the placement of a dual-chamber implantable cardioverter-defibrillator for atrioventricular block and ventricular tachycardia (VT). Clinical introduction A man in his 50s presented to the emergency department with palpitations.
Delayed-enhanced magnetic resonance imaging (DE-MRI) is useful in guiding ventricular tachycardia (VT) ablation in individuals with non-ischemic cardiomyopathy (NICM).
Ventricular tachycardia (VT) increases morbidity and mortality in patients with cardiomyopathy. Catheter ablation (CA) lowers VT recurrence and implantable cardioverter defibrillator (ICD) interventions, however, its effect on all-cause mortality remains unclear.
Wide complex tachycardia was seen on ILR tracings, and he was presumptively diagnosed with non-ischemic cardiomyopathy (NICM) and ventricular tachycardia (VT). Echo and cardiac MRI demonstrated mildly dilated left ventricle with EF 49%, no scar or ischemia.
Conclusion: Assuming none of the above exceptions exist the ECG in Figure-1 has to be presumed VT until proven otherwise. == C ASE C onclusion: Today's patient was hemodynamically stable in association with the ECG in Figure-1.
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrial fibrillation (AF), atrial flutter (AFL), and atrial tachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heart failure (HF).
Abstract Introduction Due to its unique features, pulsed field ablation (PFA) could potentially overcome some limitations of current radiofrequency (RF) ventricular tachycardia (VT) ablation. Methods Two patients with ischemic cardiomyopathy and previously failed RF VT ablations were treated with PFA.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content