This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
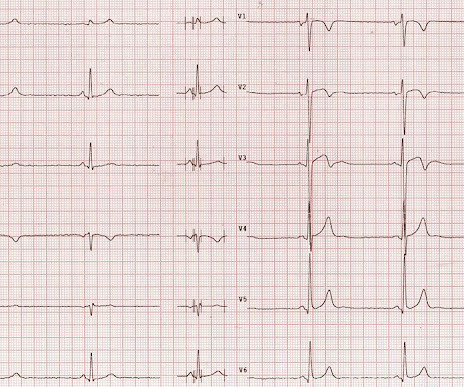
That said — the ECG in Figure-1 should prompt the following considerations: The symmetric chest lead T wave inversion in ECG #1 could be a sign of coronary disease, potentially with acute ischemia. ECG Blog #277 — Reviews findings in Takotsubo Cardiomyopathy. =
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. The patient was brought to the ED and had this ECG recorded: What do you think? And what do you want to do?
Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead. Type I ischemia. Type II ischemia.
She reports a known history of Hypertrophic Cardiomyopathy (HCM) with left ventricular outflow tract obstruction and is on daily beta blocker therapy. There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. References Naidu, S. Tower-Rader, A.
The ECG does not show any definite signs of ischemia. I thought the complete lack of QTc prolongation and anatomic localization of ECG findings made Takotsubo cardiomyopathy unlikely. The patient presented due to chest pain that was typical in nature, retrosternal and radiating to the left arm and neck. The below ECG was recorded.
Ischemic cardiomyopathy, a severe cardiac condition resulting from prolonged myocardial ischemia, is characterized by ventricular dilation, dysfunction, and an increased risk of life-threatening arrhythmias. Arrhythmia, a common complication in ischemic cardiomyopathy, is associated with poor clinical outcomes.
Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. There was hyperkinesis of the basal segments and findings were interpreted as typical of takotsubo cardiomyopathy. An MRI was deemed unnecessary at the diagnosis of stress cardiomyopathy was concidered certain. Learning points: 1.
IntroductionAcute spinal cord ischemia syndrome (ASCIS) is a rare disease that is thought to comprise roughly only 1.2% The mechanism is thought to be multifactorial due vasospasm, cerebral vasculitis, vascular thrombosis, cardioembolism from cocaine‐induced myocardial infarction or cardiomyopathy, and hypertensive surges [9].
Given her lack of risk factors for coronary disease, and the fact that she was a 53 year old woman with compatible history and echo findings, stress cardiomyopathy rose to the top of my differential. Of course, stress cardiomyopathy is a diagnosis of exclusion. This proves effective treatment of the recurrent ischemia.
My written interpretation on a tracing such as this one would read, "Marked LVH and 'strain' and/or ischemia — with need for clinical correlation." BOTTOM LINE: ECG changes of LV "strain" and/or ischemia that we see on today's initial ECG — were not present 9 years earlier. Please see ECG Blog #73 for additional details ).
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This rules out subendocardial ischemia and is diagnostic of posterior OMI. V4-5 continue to show STD.
Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. The most important clinical entity associated with motion alternans is large pericardial effusion — though motion alternans has also been observed in some cases of hypertrophic cardiomyopathy.
There is ST elevation in V2 and V3 There are inverted T-waves in V2 and V3 There are prominent U-waves in V2 and V3 Many responders were worried about ischemia or hypertrophic cardiomyopathy. This short QT at least makes ischemia all but impossible. It is only to say that the ischemia is not represented on this ECG.
And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. The fact that he has a cardiomyopathy argues for a more typical ventricular tachycardia, as does the absence of rSR' in lead V1. It is regular.
This is a very typical ECG for Hypertrophic Cardiomyopathy. The most recent previous was 4 years prior, and was in the normal range) Elderly patients, and patients with cardiomyopathy (including HOCM), may have troponin values in this range chronically ("chronic myocardial injury").
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. This suggests further severe ischemia. hours T-wave are getting larger again The patient went for an angiogram at about 7 hours after arrival.
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. CardiomyopathyCardiomyopathy is a condition that affects the heart muscle, causing it to become enlarged, thick, or rigid. This condition often leads to heart failure, as the heart cannot effectively pump blood.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients. 12:15 p.m.
The differential is: Posterolateral OMI or subendocardial ischemia The distinction between posterior OMI and subendocardial ischemia can be important and sometimes difficult. Ischemic ST depression includes posterior OMI and subendocardial ischemia. Her prior ECG on file is shown below: What are your next steps?
Arrhythmogenic cardiomyopathy Long QT syndrome Hypertrophic cardiomyopathy. There are a number of things to look for in an ECG that can hint at arrhythmia as the cause of an apparent seizure. Below are some of the conditions to be aware of: Preexcitation Brugada syndrome. I measure the RR interval at 795ms and the QT interval at 475ms.
Subsequent testing supported the presumption of apical cardiomyopathy as the cause of this patient's sustained VT. CT coronary angiogram showed no obstructive coronary disease. Today's case is illustrative because it shows how high troponin may rise despite the absence of acute coronary occlusion! (
Source: JAMA Cardiology) Patients with afib who survived an intracerebral haemorrhage had a very significant risk of cerebrovascular ischemia episodes and death in the following year, according to registry data. Patients with obstructive hypertrophic cardiomyopathy who underwent surgical myectomy reported improved quality of life.
This was my interpretation: although most ischemic T-wave inversion is post -ischemic like Wellens, sometime active ischemia results in isolated T-wave inversion. In such cases, if there is no infarction (necrosis), when the ischemia resolves, the T-wave may normalize (in contrast to Pseudo-normalize).
Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. I have summarized the m ajor e tiologic c ategories of acute myocarditis and inflammatory cardiomyopathies. She was taken to the cath lab and her coronaries were clean!! There was no MRI, but the presumptive diagnosis is myocarditis.
2020) The un-disputable fact is ischemic DCM has a target to treat, though it is termed as cardiomyopathy. The simple reason could be we can address the ischemia a potential arrhythmic target by some form of revascularization in IDCM. The second reason is, NDCM is a progressive primary muscle disease. Circulation.
remain hypo- or akinetic for some time even if not infarcted, just due to the profound ischemia incurred during the occlusive phase. Thus, an acute wall motion abnormality is not a sign of active or persistent ischemia, and thus is not necessarily an indication for emergent cath. Even many NOMI have wall motion abnormalities.
Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). The granulomatous inflammation affects the heart, causing an infiltrative cardiomyopathy The most common manifestations of cardiac sarcoidosis are atrioventricular (AV) block and ventricular tachyarrhythmias (VT).
He got an MR, however that showed no scar or evidence of AVRD and he had a stress test with no evidence of inducible ischemia with almost 20 METs." He is young and the tachycardia was not polymorphic in nature, so this is very unlikely to be an ischemic rhythm and much more likely scar mediated.
Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. If the ECG findings are truly new compared to a baseline (unavailable), this could suggest persistent ECG findings of ischemia, meaning poor downstream perfusion ("no reflow" phenomenon).
This ECG is diagnostic of diffuse subendocardial ischemia. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR.
by making it clear to everyone that this is NOT an EKG that one sees with takotsubo cardiomyopathy. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy.
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point. Again, cath lab was not activated. What does this troponin level mean?
Poor blood supply Ischemia, or inadequate blood supply to the heart, is an abnormality that can be detected in an ECG test. An ECG machine is able to detect other abnormalities of the heart as well, such as hypertrophic cardiomyopathy or overly thick heart muscles. ECG tests can also show previous heart attacks.
So cardiomyopathies, valve problems, myocarditis and previous heart attacks all cause a problem with the pumping function of the heart. These are therefore not looking for coronary disease but instead ischemia heart disease. Remember functional tests tell you about ischemia and anatomical tests tell you about coronary disease.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. LBBB is typically the result of preexisting hypertrophy, ischemic heart disease, or cardiomyopathy. 5] Isnard, R. & Pousset, F.
It may also occur in patients with underlying coronary disease, cardiomyopathy, and/or with digoxin toxicity. The other main consideration — is to take another look at the 12-lead ECG, and assess this for recent ischemia or infarction. If such subjects are asymptomatic during episodes — then no treatment is needed.
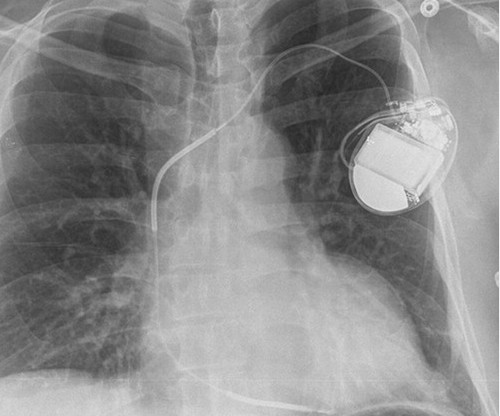
Cardiomyopathy Finally most importantly prosthetic heart valves & other Intra cardiac devices. (Most IVF pregnancies seem to need it for some unknown reason) Risk of VTE Recurrent pregnancy loss(Placental micro-circulation clogging) SLE/APLA syndrome /Scleroderma VTE related PAH Mitral valve disease with AF. What does it imply ?
Here was my answer: "Not ischemia. If not HCM — some unusual form of cardiomyopathy might explain the findings in today's ECG (ie, muscular dystrophy; infiltrative heart disease from amyloid or sarcoid; some unusual form of congenital heart disease, etc. ). This was texted to me in real time. The patient has acute chest pain.
But when the clinical presentation is sepsis, one must entertain the possibility that the ST elevation is due to demand ischemia, or some other process, and exacerbated by tachycardia. It is prudent to treat the other conditions, get the heart rate controlled, and repeat the ECG.
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. Pattern consistent with Takotsubo's cardiomyopathy." The wall motion abnormalities of Takotsubo cardiomyopathy and LAD OMI can be similar. No similar symptoms in the past. He denied headache or neck pain associated with exertion.
Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. The most important clinical entity associated with motion alternans is large pericardial effusion — though motion alternans has also been observed in some cases of hypertrophic cardiomyopathy.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content