This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
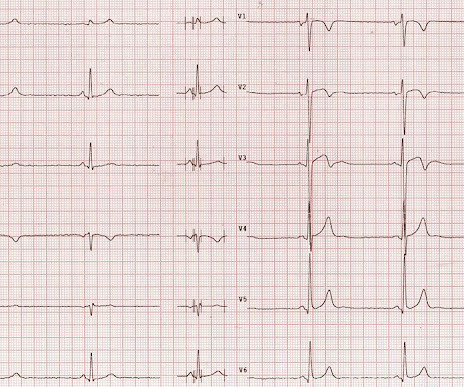
And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis.
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. CardiomyopathyCardiomyopathy is a condition that affects the heart muscle, causing it to become enlarged, thick, or rigid. This condition often leads to heart failure, as the heart cannot effectively pump blood.
My written interpretation on a tracing such as this one would read, "Marked LVH and 'strain' and/or ischemia — with need for clinical correlation." BOTTOM LINE: ECG changes of LV "strain" and/or ischemia that we see on today's initial ECG — were not present 9 years earlier. Cardiac cath showed normal coronary arteries.
There is ST elevation in V2 and V3 There are inverted T-waves in V2 and V3 There are prominent U-waves in V2 and V3 Many responders were worried about ischemia or hypertrophic cardiomyopathy. This short QT at least makes ischemia all but impossible. It is only to say that the ischemia is not represented on this ECG.
However, an echocardiogram is a different test, also conducted for heart activity. Electrocardiogram, echocardiogram, and some other tests are done for patients with cardiac arrest. Poor blood supply Ischemia, or inadequate blood supply to the heart, is an abnormality that can be detected in an ECG test.
So cardiomyopathies, valve problems, myocarditis and previous heart attacks all cause a problem with the pumping function of the heart. Overall though a normal cardiac MRI is even more reassuring than a normal echocardiogram. These are therefore not looking for coronary disease but instead ischemia heart disease.
by making it clear to everyone that this is NOT an EKG that one sees with takotsubo cardiomyopathy. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy.
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. These are reperfusion T-waves (the same thing as Wellens' waves) Echocardiogram Regional wall motion abnormality-distal septum and apex. It they are static, then they are not due to ischemia.
I have ordered an echocardiogram which will be done today, after that patient can be discharged to home with follow-up in 2 to 3 months." NOTE #3: In the context of a long QTc or ischemia — the finding of ST segment and/or T wave alternans may predict the occurrence of malignant ventricular arrhythmias. The echo was normal.
There is no evidence of infarction or ischemia. Later, he underwent a formal echocardiogram: Very severe left ventricular enlargement (LVED diameter 7.4 The absence of any wall motion abnormality makes ischemic cardiomyopathy very unlikely. There are nonspecific ST-T abnormalities. Mild to moderate mitral regurgitation.
Whenever I see PVCs with the morphology and axis seen in todays case I always look for signs of AC ( Arrhythmogenic Cardiomyopathy ). Arrhythmogenic cardiomyopathy often manifests with PVCs from the RV. The ECG in Figure-1 however, shows no signs of arrhythmogenic cardiomyopathy. Therefore A different approach is needed.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content