This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
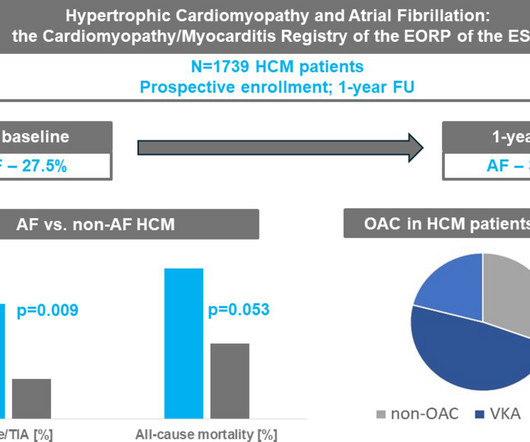
Background Hypertrophic cardiomyopathy (HCM) is commonly associated with atrial fibrillation (AF), but its impact on outcomes in real-world practice is uncertain. years) were enrolled in the EURObservational Research Programme (EORP) Cardiomyopathy/Myocarditis Registry. Methods Overall, 1739 adult patients with HCM (40.9%
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Tachycardia exaggerates ST Elevation in LBBB and Paced rhythm 5.
And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis.
Implantable cardioverter defibrillator (ICD) prevents sudden cardiac death (SCD) in patients with ischemic cardiomyopathy (ICM). Catheter ablation has been shown to effectively reduce ventricular tachycardia (VT) recurrence, yet its efficacy in patients without an ICD implantation remains uncertain.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. VF should make you think of ischemia, cardiomyopathy (especially scar from old MI), or one many other cardiac but non-ischemic etiologies. This patient was witnessed by bystanders to collapse. They started CPR. sodium bicarbonate.
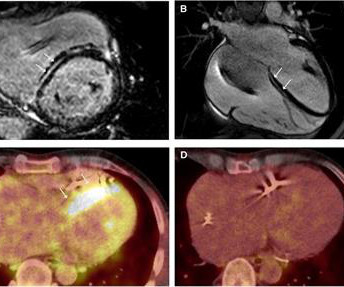
Cardiac sarcoidosis (CS), a rare condition characterized by non-caseating granulomas, can manifest with symptoms such as atrioventricular block and ventricular tachycardia (VT), as well as mimic inherited cardiomyopathies. A 58-year-old woman presented with sustained VT with a prior diagnosis of hypertrophic cardiomyopathy (HCM).
He had a background of arrhythmic right ventricular cardiomyopathy. He had previously undergone the placement of a dual-chamber implantable cardioverter-defibrillator for atrioventricular block and ventricular tachycardia (VT). Clinical introduction A man in his 50s presented to the emergency department with palpitations.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). During the next 24 hours, she experienced periods of complete AV block with a ventricular escape rhythm in the 20s. She was started on isoprenalin (isoproterenol).
The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia. Polymorphic ventricular tachycardia can be ischemic, catecholaminergic or related to QT prolongation. She spontaneously converted (Defibrillation was not performed). Takotsubo cardiomyopathy is not a completely benign disorder.
An 18-year-old male with arrhythmogenic cardiomyopathy was referred for catheter ablation of ventricular tachycardia after experiencing appropriate implantable cardioverter-defibrillator (ICD) shock. Six months prior, he had undergone uncomplicated implantation of an extravascular ICD (EV-ICD) [1].
Recent advancements in catheter ablation for structural ventricular tachycardia (VT), such as high-density mapping and cardiac imaging-based detection of target areas, have significantly improved the efficacy of ablation procedures. These developments are likely to broaden the treatment scope to include patients with recurrent VT episodes.
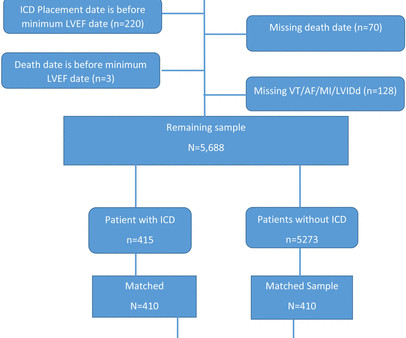
Background Consensus guidelines support the use of implanted cardioverter-defibrillators (ICD) for primary prevention of sudden cardiac death in patients with either non-ischaemic or ischaemic cardiomyopathy with left ventricular ejection fraction (LVEF) ≤35%. vs 65.4%, p<0.0001), more often white (87.5% to 1.15, p=0.482).
Progressive decline across periods in mortality rates among patients with implantable cardioverter-defibrillator (ICD). Chagas disease (ChD) was associated with increased rates of ventricular tachycardia and ventricular fibrillation in ICD patients only in the initial two periods, but there was no statistical difference in the last period.
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a disease characterised by fibrofatty replacement of the ventricular myocardium due to specific mutations, leading to ventricular arrhythmias and sudden cardiac death. Additionally, the impact of sotalol and amiodarone is inconsistent with studies reporting contradictory results.
She was successfully revived after several rounds of ACLS including defibrillation and amiodarone. An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). On arrival to the ED the patient was intubated with normal vital signs. No ischemic ST changes. Teaching Points: 1.
This can initiate ventricular arrhythmias like polymorphic ventricular tachycardia (PMVT). She was externally defibrillated with 200J and received magnesium and an IV amiodarone bolus. She was successfully defibrillated with 360J. Telemetry showed Spike-on-T phenomenon which initiated PMVT.
Ultimately the patient underwent implantation of secondary prevention implantable cardioverter-defibrillator and initiation of sotalol.Discussion:The prevalence of MAD is approximately 30% in those with MVP and 8% in the general population. Those patients with MAD and MVP appear to be at higher risk for VA and SCD.
Arrhythmogenic cardiomyopathy Long QT syndrome Hypertrophic cardiomyopathy. There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). This episode self terminated before defibrillation was possible. Potassium chloride drip was also started.
The main secondary study endpoints are all-cause mortality, cardiovascular mortality, incidence of implantable cardioverter-defibrillator (ICD) therapy, hospitalizations, quality of life, time to first ICD therapy, number of device-detected ventricular tachycardia/ventricular fibrillation episodes, left ventricular function, and exercise tolerance.
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This prompted cath lab activation. On arrival to the ED, this ECG was recorded: What do you think?
After resuscitation and defibrillation , there were no more episodes of TdP. Below is the patient’s 12 lead ECG following defibrillation. The patient was diagnosed with stress cardiomyopathy. Widespread T wave inversions and prolongation of the QT interval is not uncommon in Takotsubo cardiomyopathy.
From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. McLaren : We’ve answered the first question – Sinus Tachycardia with episodic runs of wide QRS (RBBB morphology) and PVC’s.
The deep learning algorithm helps segment the left ventricle predicting cardiomyopathy and ejection fraction. Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia.
ABSTRACT Cardiomyopathies are a significant contributor to cardiovascular morbidity and mortality, mainly due to the development of heart failure and increased risk of sudden cardiac death (SCD). Despite improvement in survival with contemporary treatment, SCD remains an important cause of mortality in cardiomyopathies.
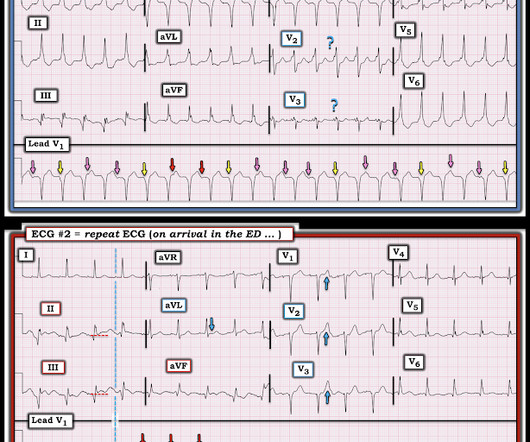
This proves AV dissociation, and by extension ventricular tachycardia. The note lists a diagnosis of "tachycardia," which is described as "narrow complex." (The Repeat ECG obtained in ER: Fortunately for the patient, his ventricular tachycardia spontaneously resolved. Documentation lists a diagnosis of "sinus tachycardia."
Repeat ECG was obtained immediately, just 24 minutes after the prior ECG: Given the context, my top differential diagnosis would be stress cardiomyopathy AKA takotsubo. In my opinion, the more likely explanation is that the ST-T changes are primarily driven by stress cardiomyopathy. She was defibrillated perhaps 25 times.
There was never ventricular fibrillation (VF) or ventricular tachycardia (VT), no shockable rhythm. By ECG alone: it is suspicious for stress cardiomyopathy, or takotsubo, due to the diffuse ST Elevation: II, III, aVF AND I and aVL. Here is a similar case: Collapse, Ventricular Tachycardia, Cardioverted, Comatose on Arrival.
Smith comments : Wide complex tachycardia. The differential diagnosis of WCT is: 1) Sinus tachycardia with "aberrancy" (in this case RBBB and LAFB), but there are no P-waves and the QRS morphology is not typical of simple RBBB/LAFB. Also, if the rate is constant, not wavering up and down, it is highly unlikely to be sinus tachycardia.
Whenever I see PVCs with the morphology and axis seen in todays case I always look for signs of AC ( Arrhythmogenic Cardiomyopathy ). Arrhythmogenic cardiomyopathy often manifests with PVCs from the RV. The ECG in Figure-1 however, shows no signs of arrhythmogenic cardiomyopathy.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content