This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. They started CPR.
And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis.
She spontaneously converted (Defibrillation was not performed). Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. There was hyperkinesis of the basal segments and findings were interpreted as typical of takotsubo cardiomyopathy. Below is the ECG one month after discharge.
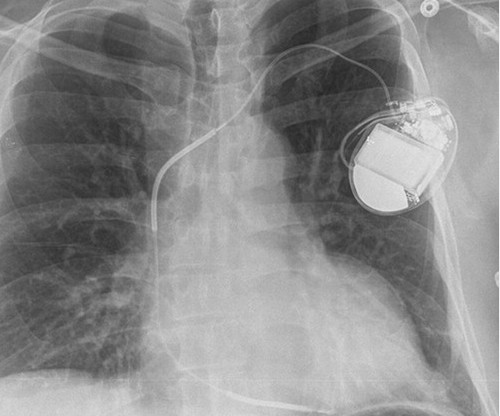
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. CardiomyopathyCardiomyopathy is a condition that affects the heart muscle, causing it to become enlarged, thick, or rigid. Implantable Cardioverter-Defibrillator (ICD) to help manage dangerous heart rhythms.
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This rules out subendocardial ischemia and is diagnostic of posterior OMI. V4-5 continue to show STD.
She was successfully revived after several rounds of ACLS including defibrillation and amiodarone. Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. On arrival to the ED the patient was intubated with normal vital signs.
Tackling SCD was in God’s domain, until the brilliance of Dr. Michel Mirowski shrunk the defibrillator and implanted it under the chest in 1980. (Dr. 2020) The un-disputable fact is ischemic DCM has a target to treat, though it is termed as cardiomyopathy. SCD is the leading cause of mortality in heart failure. N Engl J Med.
Arrhythmogenic cardiomyopathy Long QT syndrome Hypertrophic cardiomyopathy. This episode self terminated before defibrillation was possible. There are a number of things to look for in an ECG that can hint at arrhythmia as the cause of an apparent seizure. I measure the RR interval at 795ms and the QT interval at 475ms.
Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). Discussion : The initial ECG in today's case is pathological for any patient, especially for a 50-year old previously heathy female.
She was never seen to be in ventricular fibrillation and was never defibrillated. This ECG is diagnostic of diffuse subendocardial ischemia. Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. With ventilations and epinephrine, she regained a pulse. BP gradually rose.
She was defibrillated and resuscitated. by making it clear to everyone that this is NOT an EKG that one sees with takotsubo cardiomyopathy. The impact of ST-segment elevation on the prognosis of patients with Takotsubo cardiomyopathy. Smith: this ECG and clinical presentation is diagnostic of LAD Occlusion.
Repeat ECG was obtained immediately, just 24 minutes after the prior ECG: Given the context, my top differential diagnosis would be stress cardiomyopathy AKA takotsubo. It is possible there is microvascular dysfunction producing residual transmural ischemia. She was defibrillated perhaps 25 times. We will never know for certain.
By ECG alone: it is suspicious for stress cardiomyopathy, or takotsubo, due to the diffuse ST Elevation: II, III, aVF AND I and aVL. Subarachnoid hemorrhage causes extreme central catecholamine output, resulting in stress cardiomyopathy, just like takotsubo. This is unusual in acute OMI. she had severe pulmonary edema.
Whenever I see PVCs with the morphology and axis seen in todays case I always look for signs of AC ( Arrhythmogenic Cardiomyopathy ). Arrhythmogenic cardiomyopathy often manifests with PVCs from the RV. The ECG in Figure-1 however, shows no signs of arrhythmogenic cardiomyopathy. Therefore A different approach is needed.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content