This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Getty Images milla1cf Tue, 05/14/2024 - 13:00 May 14, 2024 — One of the most common genetic heart diseases worldwide, hypertrophic cardiomyopathy (HCM) causes the walls of the left ventricle to become thick and stiff. The late breaking research was presented by principal investigator Martin S.
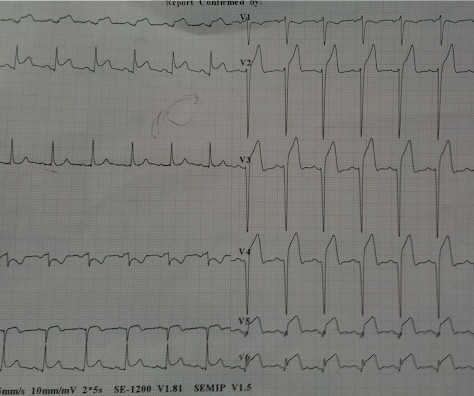
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. This is a very typical ECG for Hypertrophic Cardiomyopathy. I was reading ECGs on the system and saw this one, and instantly knew the probable ECG diagnosis: What do you think? What do you think now?
Takotsubo Stress Cardiomyopathy that mimics LAD occlusion Cath was clean. Takotsubo Typical Takotsubo, very unlikely to be ACS because of extremely long QT Presented with altered mental status, hypotension, and mild chest discomfort Peak trop 0.15 Diffuse ST Elevation with Apical Ballooning: is it Takotsubo Stress Cardiomyopathy?
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. Stress induced cardiomyopathy (Takotsubo like LV dysfunction) possible The appearance of wall motion abnormalities in some apical views suggest possibility of stress mediated cardiomyopathy. What do you think?
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Pretest probability: Especially when there is no Chestpain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear.
Submitted by anonymous, written by Pendell Meyers A woman in her 50s presented to the Emergency Department with chestpain and shortness of breath that woke her from sleep, with diaphoresis. See these other cases of arterial pulse tapping artifact: A 60 year old with chestpain Are these Hyperacute T-waves?
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chestpain and shortness of breath after finishing a 4-mile run. His symptoms of chestpain and shortness of breath were attributed to an asthma exacerbation during exercise.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
This ECG was texted to me with the words "Cocaine" and "Chestpain." This ECG was recorded at 82 minutes: No Evolution; this supports absence of OMI Troponin I (hs) were: 0 hour: 7 ng/L, 2 hour: 9 ng/L, 4 hour: 8 ng/L (Rules out Acute MI) Thus, the chestpain was non-ischemic. There are QS-waves in V1 and V2.
A 63-year-old woman presents to the office for a second opinion on chronic chestpain and heart failure management. She has a medical history of mixed connective tissue disease, obstructive sleep apnea, hepatic steatosis, and long-standing hypertension diagnosed in her twenties.
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chestpain without radiation or dyspnea. She felt nauseous and lightheaded with no neurologic deficits.
The patient has acute chestpain. If not HCM — some unusual form of cardiomyopathy might explain the findings in today's ECG (ie, muscular dystrophy; infiltrative heart disease from amyloid or sarcoid; some unusual form of congenital heart disease, etc. ). This was texted to me in real time. What do you think?
Takotsubo cardiomyopathy is also a possible explanation. An echo was done and decision was made to pursue cath lab the following day as the echocardiography was interpreted as consistent with Takotsubo Cardiomyopathy. Maybe it is T wave inversion of Takotsubo Cardiomyopathy ? There was never any severe chestpain.
Seventeen patients hospitalized for suspected hot-phase cardiomyopathy underwent both endomyocardial biopsy (EMB) and genetic testing: histological detection of apoptosis at EMB was frequent (77% of cases) and all patients that tested positive for pathogenic/likely pathogenic variants showed apoptosis at EMB.
He presented with chestpain, not relieved by nitro, pain reproducible on exam and centered around the pacemaker insertion site. Here is his ECG one month prior, on admission for chestpain at that time also: Similar ratios. It is likely that severe cardiomyopathy and loading conditions result in false positives.
She reports a known history of Hypertrophic Cardiomyopathy (HCM) with left ventricular outflow tract obstruction and is on daily beta blocker therapy. Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. Below are two examples of this.
BackgroundSigmoid Ventricular Septum (SVS) is a type of hypertrophic cardiomyopathy characterized by a reduced angle between the basal interventricular septum and the ascending aorta, and SVS can lead to dynamic Left Ventricular Outflow Tract obstruction (LVOTO) during hypercontractile states.
Just as important is pretest probability: did the patient report chestpain prior to collapse? VF should make you think of ischemia, cardiomyopathy (especially scar from old MI), or one many other cardiac but non-ischemic etiologies. After cardiac arrest, I ALWAYS wait 15 minutes after an ECG like this and record another.
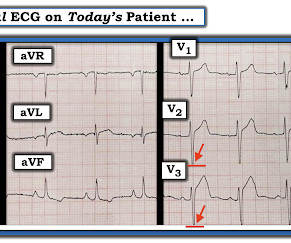
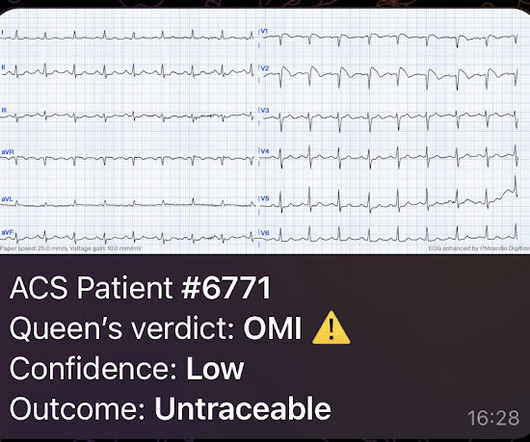
As noticed by the AI, if the patient presented with chestpain , then even this subtle ECG is diagnostic of OMI. What do you think? Here's what the Queen of Hearts thinks: Note that the Queen has "HIGH" confidence that this is OMI.
The chestpain quickly subsided. There was hyperkinesis of the basal segments and findings were interpreted as typical of takotsubo cardiomyopathy. An MRI was deemed unnecessary at the diagnosis of stress cardiomyopathy was concidered certain. Takotsubo cardiomyopathy is not a completely benign disorder.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chestpain: V5 and V6 sure look like a STEMI For this ECG and chestpain in the ED, the Cath lab activated. But the angiogram was clean.
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. The fall was not a mechanical etiology. He denied any specific prodrome of gross palpitations, however did endorse feeling quite dizzy just before the event.
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Pretest probability: Especially when there is no Chestpain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear.
(In other words, the artery was occluded but has sponteneously reperfused, resulting in pain relief) It is important to monitor patients with Wellens' syndrome for re-occlusion, which is usually, but not always, associated with recurrent chestpain. The patient remained pain free. ChestPain scores can be misleading.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chestpain. He has "ischemic cardiomyopathy" and "congestive heart failure." He had no h/o heart failure. Here is the next day ECG: Some posterior reperfusion T-waves (slightly larger upright T-waves in V2 and V3).
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Here is the clinical informaton on ECG 2: A man in his 50s presented to the Emergency Department with acute chestpain that started within the past few hours.
She asked me why I felt she had had a heart attack and I explained to her that she had had chestpains and the blood test indicating damage to the heart was elevated and that was all we needed to say that she had had a heart attack. On the basis of these findings we told her that she had suffered a heart attack.
As discussed in detail in ECG Blog #228 — this seemingly qualifies as a “ Silent ” MI ( Approximately half of those MIs not accompanied by CP — have some other associated symptom such as syncope, which substitutes as a “chestpain equivalent” ). Longterm prognosis of patients with MINOCA clearly depends on the underlying etiology.
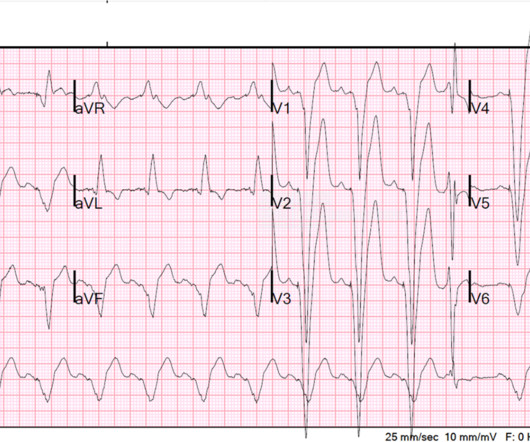
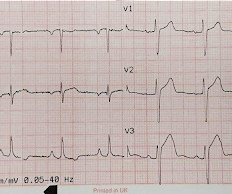
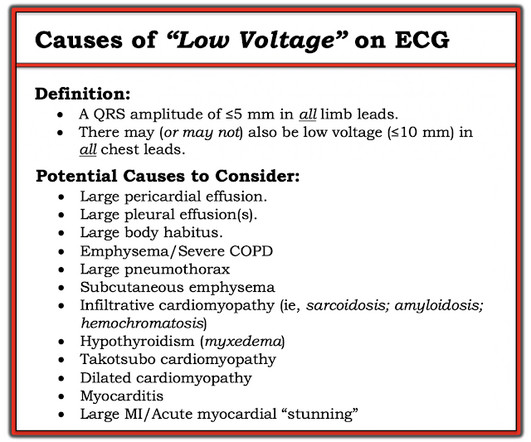
This middle aged patient presented with chestpain: What do you think? There is VERY low voltage. There is some ST Elevation, but it is MINIMAL. But look how small the QRS is!! Let's stretch out the QRS vertically so it is not so tiny: On upper left is the original. As shown in Figure-2 — there are other entities to consider!
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
On the other hand — the ST elevation seen in lead V1 is perfectly consistent with LVH and LV "strain" ( ie, The shape of this ST-T wave in lead V1, in association with the deep S wave in this lead — is a mirror-image opposite picture of the typical expected appearance of LVH with "strain" in a lateral chest lead ).
The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chestpain. 2-3 days after this he developed the same sharp chestpain and shortness of breath with elevated inflammatory markers (CRP) as well as typical findings of pericarditis seen on ECG.
Yes, COVID-19 symptoms can resemble a heart attack, including chestpain, shortness of breath, and changes in echocardiogram or EKG. It serves as an initial assessment, and an MRI may be considered if other signs of cardiomyopathy are present. Can COVID-19 symptoms mimic a heart attack?
The patient's chestpain had resolved by the time of the ECG 2. But it does prove that the patient has coronary disease and makes the probability that his chestpain is due to ACS very very high. He presents with an episode of brief, new-onset chestpain that had resolved by the time E CG # 1 was obtained.
No chestpain. Figure-1: The initial ECG in today's case — obtained from an 86-year old man with presyncope, but no chestpain. ( It may also occur in patients with underlying coronary disease, cardiomyopathy, and/or with digoxin toxicity. Th e patient was hemodynamically stable in association with this rhythm.
RVOT VT: A 40-something without past history presents with wide complex tachycardia and crushing chestpain Regular Wide Complex Tachycardia. No , this requires inferior axis and LBBB morphology. There is no inferior axis. What is the Diagnosis? Figure-1: The initial ECG that was recorded in the ED.
Subsequent testing supported the presumption of apical cardiomyopathy as the cause of this patient's sustained VT. ie, Severe subendocardial ischemia from sustained VT in a patient severe apical cardiomyopathy resulted in a peak troponin >31,000 ng/L in today's case ). CT coronary angiogram showed no obstructive coronary disease.
While fully acknowledging that "Sometimes ya gotta be there!" — in order to optimally assess the patient — the clinical definition of hemodynamic stability is for the patient to be without significant symptoms such as chestpain, shortness of breath, hypotension and/or mental status changes — as a direct result of the fast heart rate.
Case 2: sent by Dr. James Alva A man in his 50s with diabetes, hypertension, and hyperlipidemia presented to the ED with chestpain and shortness of breath off and on over the past three days, with associated vomiting. M y T HOUGHTS on E CG # 1 — The patient in Case #1 was a 60-something woman with acute dyspnea, but no chestpain.
Troponins may be negative with very rapid reperfusion, or measured too late, or chronically elevated due to cardiomyopathy or renal failure. While ST coving in V1 is not necessarily abnormal — the presence of ST elevation in association with ST-T wave abnormalities in V2,V3 in a patient with chestpain is clearly cause for concern.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content