This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Henry Ford Health's National CardiogenicShock Initiative research team. Cardiogenicshock is a critical condition in which the heart is unable to pump enough blood to sustain the body’s needs, depriving vital organs of blood supply. This can cause those organs to eventually stop functioning.
Introduction The use of contemporary drug-eluting stents (DES) has significantly improved outcomes of patients with coronary artery disease (CAD) undergoing percutaneous coronary intervention (PCI). Patients with left main (LM) disease, cardiogenicshock (CS), or severely reduced left-ventricular ejection fraction (LVEF) were excluded.
Now appears to be in cardiogenicshock." However, cardiogenicshock usually takes some time to develop, so it is probably subacute." Cardiogenicshock and ACS is an indication for the cath lab, even if you don't think there is OMI. I was texted these ECGs. Then SOB and nausea the next day.
Past medical history includes coronary stenting 17 years prior. If you take old people with a history of MI (he had a stent), that percentage goes far higher since there is scar tissue that acts as a nidus for the PVCs that initiate VT. He had concurrent sharp substernal chest pain that resolved, but palpitations continued.
She arrived comatose and in cardiogenicshock and the following ECG was recorded. Pressors were required, and the patient was transported to the cath lab with a door to balloon time of 60 minutes, where a proximal dominant RCA occlusion was opened and stented. She was intubated.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The notes now refer to the patient being in cardiogenicshock, on pressors. Am J Emerg Med. 2014;32:e5–e8. J Cardiol Cases.
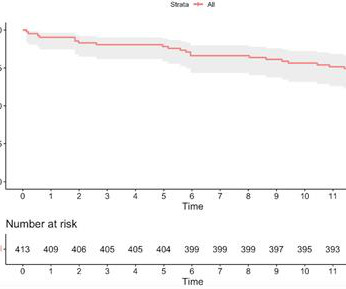
Intra-procedural data included access route, coronary anatomy, lesion complexity, number of stents deployed, door-to-balloon time for primary PCI, and any intra-procedural complications. and the average number of stents 2.6. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenicshock. She was worked as a full code, and ROSC was achieved. Later the next day, she went into cardiac arrest again.
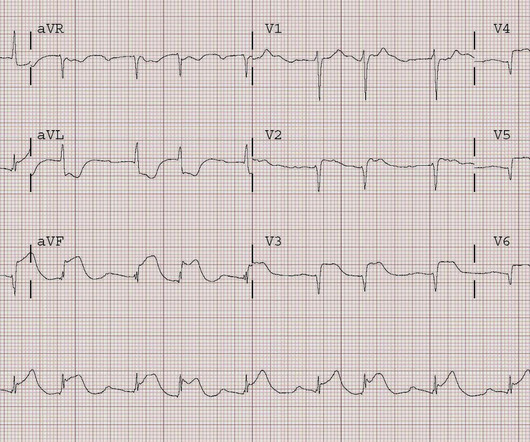
The patient was referred immediately for cath which revealed RCA occlusion that was stented. The patient died of cardiogenicshock within 24 hours despite mechanical circulatory support. There is some down sloping ST-segment and T wave inversion in lead aVL. The findings are diagnostic of inferior and posterior wall OMI.
So the RCA was stented. The patient continued to have chest pain after the RCA was reperfused, so the LAD was then stented. But by this time the patient went into cardiogenicshock and passed away.
P.S.: Cardiac cath was performed — and showed a distal LA D "culprit" lesion that was successfully stented. Unfortunately — this patient died within 12 hours of obtaining this tracing from cardiogenicshock. The above said, this is not Wellens' Syndrome — because a large infarction has already occurred! (
The patient is started on epinephrine infusion for cardiogenicshock and cardiology took the patient to the cath lab. Two stents were placed with resultant TIMI 3 flow. The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria.
Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. However, raising the pulse to 60 is hardly "working" for a patient who needs a lot more cardiac output. Fortunately, the patient made it to the cath lab alive without pacing or intubation.
He was taken to the cath lab where he was found to have acute total occlusion of his saphenous vein graft to his RCA, which was stented. He was in cardiogenicshock requiring an impella for several days after cath. No further troponins were measured.
Why is the patient in shock? He was in profound cardiogenicshock. He was successfully stented. There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI).
TIMI flow 0) is rare in the ED, as most either die before arrival or are recognized clinically due to cardiogenicshock. 67) Less than 3% of anterior STEMI has LM OMI, and most are recognized clinically due to cardiogenicshock. (68, Everolimus-Eluting Stents or Bypass Surgery for Left Main Coronary Artery Disease.
So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent. Queen of Hearts interpretation: Now the cardiologist considered it "STEMI"!
distal stent patent. The patient went into cardiogenicshock and ultimately died of this MI. Repeat ECG shows modest ST elevation in I and aVL and depression in inferior leads." The cath lab was activated. Angiogram: LM 30% ostial. LAD 80% mid LCx occluded mid (acute infarct lesion) RCA 80% mid.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenicshock" is not applicable outside of sinus rhythm. However we also noticed that the rhythm is rapid, regular, and narrow, with no P-waves, at a rate of approximately 200 bpm, and therefore not sinus rhythm in this patient in his 60s.
A completely blocked artery is located, a wire is inserted through it, the clot is sucked, the narrowing is widened with a balloon, and then a stent (stainless steel wire mesh) is placed to maintain consistent flow. It’s essential for those at risk of coronary artery disease to be aware of the following symptoms.
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The Society (..)
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
He had undergone stenting of the LAD several weeks ago (unclear whether elective for stable symptoms, or in response to acute coronary syndrome). That the chief complaint of today's patient was acute CP ( C hest P ain ) with a history of known coronary disease and LAD stent placement a few weeks earlier. He appeared critically ill.
A 2017 trial named CULPRIT SHOCK found that in patients with cardiogenicshock, a strategy of culprit vessel PCI only was associated with better outcomes than immediate multivessel PCI. After CULPRIT SHOCK, many shied away from multivessel PCI in the acute setting. In fact, in this elegant study by Heitner et al.
24) Microaxial Flow Pump in Infarct-Related CardiogenicShock DanGer Shock (ACC.24) It is asking for stenting all non-flow limiting lesion , if found, to carry high risk plaques by intracoronary Imaging. Top 10 Clinical Trials Preventive PCI on Stenosis With Functionally Insignificant Vulnerable Plaque PREVENT (ACC.24)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content