This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
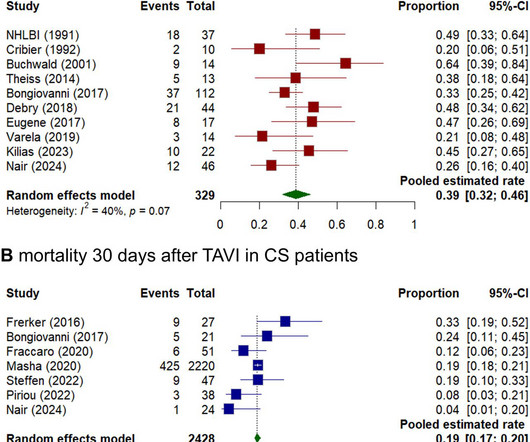
Background Cardiogenicshock (CS) induced by severe aortic stenosis (AS) is a life-threatening condition with high mortality. Despite advancements in emergency interventions, the optimal treatment approach remains uncertain.
What is the preferred order of vasopressors and ionotropes in the management of cardiogenicshock? How can we best pick up occult cardiogenicshock before it floured shock kicks in? The post Ep 164 CardiogenicShock Simplified appeared first on Emergency Medicine Cases.
A nationwide observational analysis of patients with aortic stenosis (AS) and cardiogenicshock (CS) who underwent transcatheter aortic valve replacement (TAVR) or surgical aortic valve replacement (SAVR) determined that patients who underwent TAVR had lower in-hospital complications and resource utilization compared with SAVR.
In acute heart failure caused by VHD, symptoms result from rapid haemodynamic changes and subsequent decline in cardiac function, and if left untreated, leads to acute decompensation and cardiogenicshock. After screening a total of 2234 articles, 76 published between 1994 and 2023 were included in subsequent analysis.
Now appears to be in cardiogenicshock." However, cardiogenicshock usually takes some time to develop, so it is probably subacute." Here I annotate it: This shows 100% occluded circumflex (red arrow) and a 90% stenosis of the LAD (Yellow arrow). I was texted these ECGs. Then SOB and nausea the next day.
A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. The aortic valve in this example also had critical stenosis by Doppler The patient continued to be hemodynamically unstable with poor cardiac output and very high LV filling pressures.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Category 2 : An increase in myocardial oxygen demand due to tachycardia, elevated ventricular afterload (BP or aortic stenosis), or increased wall stretch (admittedly this latter is more complicated) or a decrease in oxygen supply due to hypotension, anemia, hypoxia, or a combination of all of the above. Aortic Stenosis f.
COPD, Idiopathic PAH, acute or chronic PE, pulmonary valve stenosis, etc) 3) Conditions affecting RV myocardial contractility, such as ARVD or RV infarction The ECGs does not really show any signs of chronic RV dilation or hypertrophy. Any cause of pulmonary hypertension. Our THANKS to Dr. Magnus Nossen for sharing this case with us.
Just prior to transport, the patient became confused and agitated and, although blood pressure and pulse were OK, I was worried about cardiogenicshock. Angiogram Left main: Severe calcific stenosis of ostial and distal left main. LAD: large caliber vessel with severe calcific stenosis of the proximal LAD with TIMI2 flow.
History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. An elderly man with sudden cardiogenicshock, diffuse ST depressions, and STE in aVR Literature 1. Left main?
Figure B At this point, with the ECG changing from diffuse ST depression to widespread ST elevation and the patient presenting in cardiogenicshock, left main coronary artery (LMCA) occlusion is the likely diagnosis. Below is a still image with the red arrow indicating the subtotal LMCA stenosis. This is an ominous sign.
Angiography : LMCA — 90-99% osteal stenosis. LCx — 50-69% stenosis of the 1st marginal branch; with 100% distal LCx occlusion. The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. RCA — 100% proximal occlussion.
He was taken rapidly to the cath lab and here are some representative images before and after intervention: Acute proximal LAD culprit with TIMI 0 flow, 100% stenosis, thrombotic occlusion, requiring thrombectomy and PCI. Post cath EF was estimated at 15% with severe global hypokinesis, and akinesis of the apex.
Why is the patient in shock? He was in profound cardiogenicshock. He was taken to the cath lab and underwent emergent intervention: Thrombotic stenosis of the proximal RCA (95% with evidence of plaque rupture) is the culprit for the patient's inferoposterior STEMI. There is an obvious inferior STEMI, but what else?
61,62) The interventional community defines occlusive LM disease as >50% by FFR, or ≥75% stenosis,(63) but urgent or emergent intervention on lesions not meeting these thresholds is only imperative if it is a thrombotic lesion and the patient has refractory ischemic symptoms (i.e. TIMI 0/1 flow).(61,62) Knotts et al.
The patient is started on epinephrine infusion for cardiogenicshock and cardiology took the patient to the cath lab. Angiogram showed a culprit lesion of 100% stenosis to the right coronary artery and 100% stenosis of the right posterior descending artery, both with TIMI 0 flow.
Tachycardia is unusual for OMI, unless the patient is in cardiogenicshock (or getting close). In addition, the top left blue arrow indicates a section in the LAD with a severe stenosis, likely the culprit for the prior L A D occlusion which has since recanalized. There are also diagonal branches which are not well visualized.
So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent. Queen of Hearts interpretation: Now the cardiologist considered it "STEMI"!
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-Arterial Coronary Surgery: Ten Year Follow-up of One Million (..)
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
Mind you, IABP during cardiogenicshock, essentially does this – keep the coroanry diastolic pressure high. FFR during exertion typically decreases compared to rest due to the amplified pressure gradient across the stenosis driven by increased flow demand and limited reserve.However collaterals can mitigate this fall in FFR.
Whenever there is tachycardia, I am skeptical of OMI unless it has led to severely compromised ejection fracction with cardiogenicshock. Smith : "decompensation" of aortic stenosis might have initiated this entire cascade. What "initiates" the aortic stenosis cascade? We certainly know that there is hypoxia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content