This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. At first glance, it seems the patient is having a STEMI. Then ACS (STEMI) might be primary; this might be cardiogenicshock.
A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenicshock. Here was the ECG: There is sinus tachycardia. So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? This was sent by a reader. and K was normal.
Here are more examples of wide complex tachycardia: these are all a mix of ventricular tachycardia and SVT with aberrancy. He was in cardiogenicshock. There is tachycardia, and there is a wide complex. This wide complex tachycardia could easily be misdiagnosed as V tach.
Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? The VSR is what is causing the cardiogenicshock! She had a very elevated troponin T at 12,335 ng/L at the time of presentation.
The conventional machine algorithm interpreted this ECG as STEMI. It shows sinus tachycardia with right bundle branch block. Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenicshock). When EMS found her, she was dyspneic and diaphoretic.
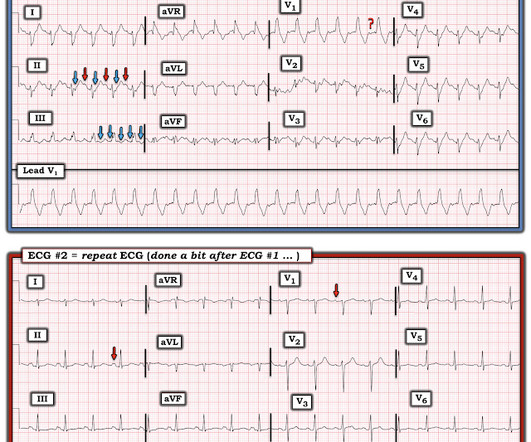
when the usual negative P wave deflection of sinus tachycardia is nowhere to be found in lead V1 )? While of course possible for the rhythm in ECG #1 to be either AFlutter or fascicular VT — sinus tachycardia immediately becomes a much more likely possibility once we know that this patient is critically ill with multisystem disease.
Because of the tachcardia, I would expect her to be very poor left ventricular function and maybe Cardiogenicshock. Still Irregular Blood pressure during these rhythms was adequate; there was no shock. The patient spontaneously converted back to sinus tachycardia. Later, I obtained more clinical history.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
There is sinus tachycardia (do not be fooled into thinking this is VT or another wide complex tachycardia!) This pattern is essentially always accompanied by cardiogenicshock and high rates of VT/VF arrest, etc. The patient arrived to the ED in cardiogenicshock but awake. Code STEMI was activated.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. Authors' commentary: Cardiogenicshock in the setting of severe aortic stenosis. What do you see?
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenicshock" is not applicable outside of sinus rhythm. 2) Tachycardia to this degree can cause ST segment changes in several ways. Is that an obvious STEMI underneath that rhythm?
There is sinus tachycardia. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology. I have always said that tachycardia should argue against acute MI unless there is cardiogenicshock or 2 simultaneous pathologies. Here is that ECG: What do you think?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
There is an obvious inferior STEMI, but what else? Why is the patient in shock? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. He was in profound cardiogenicshock. This STE is diagnostic of Right Ventricular STEMI (RV MI). A right sided ECG was not recorded.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
Assessment was severe sudden cardiogenicshock. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 They recorded an EC G: New ST Elevation.
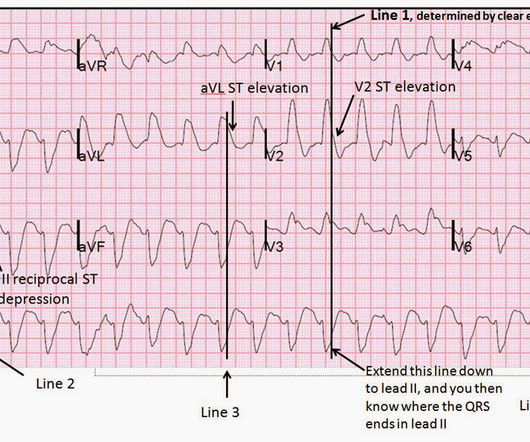
It is a wide complex regular tachycardia at a rate of 120. Is it ventricular tachycardia? I fear that many learners would also not easily recognize where the QRS actually ends, and I fear that some may think that this is ventricular tachycardia due to inability to distinguish QRS from ST segment. The ST Elevation is NOT typical.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. However, there is also significant tachycardia , with heart rate of 116, and known hypoxia. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). An EKG was immediately recorded.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content