This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
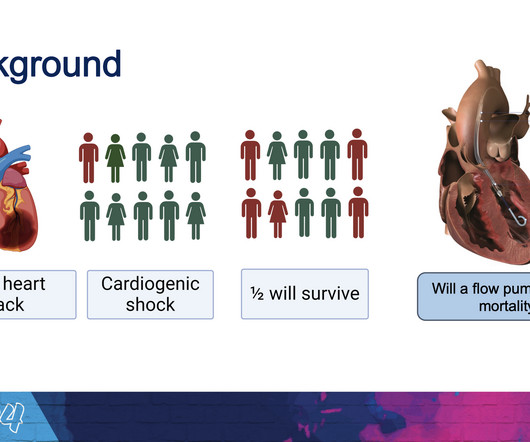
(MedPage Today) -- ATLANTA -- Routine use of the Impella CP microaxial flow pump significantly improved survival in patients with infarct-related cardiogenicshock, the randomized DanGer Shock trial showed. In more than 350 patients receiving.
The goal of the DanGer Shock trial was to compare the safety and efficacy of Impella CP on top of standard care compared with standard care alone among patients with ST-segment elevation myocardial infarction (STEMI) and cardiogenicshock.
Implantation of the Impella CP micro-axial flow pump may increase survival at six months among patients with STEMI complicated by cardiogenicshock (CS), according to the results of the DanGer Shock study.
Cardiogenicshock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset How is CS in NSTEMI different ?
Nature Reviews Cardiology, Published online: 23 April 2024; doi:10.1038/s41569-024-01035-9 Data from the DanGer Shock trial demonstrate that implantation of a microaxial flow pump in patients with ST-segment elevation myocardial infarction complicated by cardiogenicshock increases the survival rate compared with standard care alone.
An exploratory analysis of randomized data demonstrates higher mortality and less clear benefit of mAFP use in older patients with STEMI-related cardiogenicshock.
Introduction Cardiogenicshock (CS) complicates 5%–15% of cases of acute myocardial infarction (AMI) with inpatient mortality greater than 40%. This prospective registry includes all patients >18 years of age presenting with STEMI with or without CS beginning on 1 February 2023.
A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenicshock. So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? This was sent by a reader. and K was normal. Here was the ECG: There is sinus tachycardia.
Here is the Queen of Hearts (version 1) interpretation: Click here to sign up for Queen of Hearts Access Angiogram images before and after intervention: Another view (before and after intervention): The patient was confirmed to be in cardiogenicshock, placed on ECMO, also with impella assist device.
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. At first glance, it seems the patient is having a STEMI. ACS and STEMI generally do not cause tachycardia unless there is cardiogenicshock.
Now appears to be in cardiogenicshock." However, cardiogenicshock usually takes some time to develop, so it is probably subacute." This can only be due to STEMI. Cardiogenicshock and ACS is an indication for the cath lab, even if you don't think there is OMI. I was texted these ECGs.
The VSR is what is causing the cardiogenicshock! It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. PIRP is strongly associated with myocardial rupture. PIRP was associated with persistent upright T waves.
Older patients with STEMI-related cardiogenicshock have a greater risk of mortality and may not experience the same benefit from microaxial flow pump (mAFP) treatment as their younger counterparts, according to an exploratory secondary analysis of the DanGer Shock trial presented at AHA 2024 and simultaneously published in JACC.
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardial infarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients. 3.45) and 4.47 (95% CI: 2.54–7.87),
The conventional machine algorithm interpreted this ECG as STEMI. Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenicshock). See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Both were wrong.
Subtle as a STEMI." (i.e., A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenicshock. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. This one is easy for the Queen.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. Authors' commentary: Cardiogenicshock in the setting of severe aortic stenosis. What do you see?
Clinical presentation was stable angina 130/567 (22.9%), non-ST-elevation acute coronary syndrome (NSTEACS) 312/567 (55%), ST-elevation myocardial infarction (STEMI) 125/567 (22.0%), and STEMI with cardiogenicshock 13/125 (10.4%). The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch. What is the atrial activity? Is it sinus arrest with junctional escape?
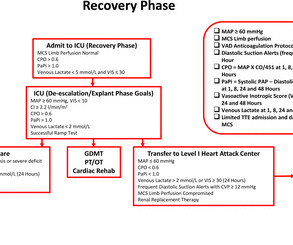
Troponin T peaked at 2074 ng/L (very high, typical of OMI/STEMI). Post PCI the patient became gravely hypotensive and "shocky". She stabilized on dobutamine and levosimendan infusions that could be discontinued after 24 hours. The tricuspid annular plane systolic excursion (TAPSE) improved from 15mm to 19mm within the first 24 hours.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). The notes now refer to the patient being in cardiogenicshock, on pressors.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
Then the notes mention "cardiogenicshock" but without any reference to a cardiac echo or to a chest x-ray. Cardiologist note says: "Elevated troponin explained by type II MI due to her shock." Trop T now very high, well into the range one sees with a STEMI; very unusual in type II MI. Was there pulmonary edema?
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. But by this time the patient went into cardiogenicshock and passed away.
When the ST vector is primarily posterior, the diagnosis is usually posterior STEMI. ST depression maximal in V5 and V6 cannot be reciprocal to subepicardial, transmural ischemia under aVR because, as stated above, there is no ventricular myocardium beneath that lead, no STEMI under aVR. I just read Ken's comments before publishing.
I have always said that tachycardia should argue against acute MI unless there is cardiogenicshock or 2 simultaneous pathologies. Exclusion criteria were age less than 18, SBP less than 100 mmHg, echocardiogram with EF less than 50%, STEMI, pregnancy, and trauma. PR depression, which suggests pericarditis 4.
A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al. were pretty sick, with mostly LM/pLAD lesions and high rates of cardiogenicshock. I had no idea SCAD was so common a cause of acute STEMI in younger women, even when they are non-smokers.
Because of the tachcardia, I would expect her to be very poor left ventricular function and maybe Cardiogenicshock. Dyspnea, Right Bundle Branch block, and ST elevation Here are two more cases where the differential diagnosis is acute OMI vs. LV aneurysm: Is this acute STEMI? Not all anterior LV aneurysm has a QS-wave.
He was in cardiogenicshock requiring an impella for several days after cath. No further troponins were measured. He was taken to the cath lab where he was found to have acute total occlusion of his saphenous vein graft to his RCA, which was stented.
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. So the cath lab was activated. Long term outcome is unavailable.
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
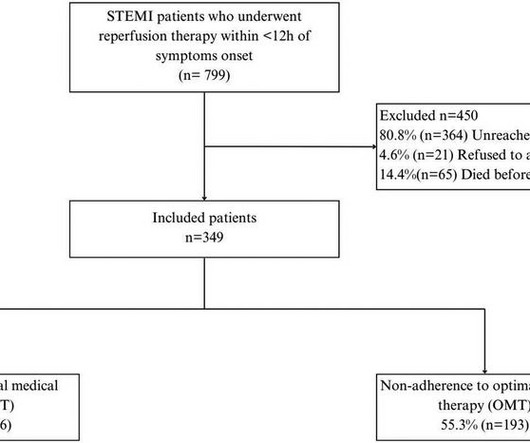
IntroductionIn developing countries, there is a notable scarcity of real-world data on adherence to optimal medical therapy (OMT) and its correlation with major cardiovascular adverse events (MACEs) after ST-elevation myocardial infarction (STEMI). Patients were followed up for 4.5 ResultsWe included 349 patients with a mean age of 58.08
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria. Do you think we discussed this patient's 2-3 hour delay to reperfusion in our quarterly "STEMI meeting"?
milla1cf Mon, 04/08/2024 - 18:07 April 8, 2024 — Implantation of the Impella CP micro-axial flow pump in the hours after a heart attack significantly increased the rate of survival at six months among people suffering cardiogenicshock, according to a study presented at the American College of Cardiology ’s Annual Scientific Session.
He was in cardiogenicshock. As you will see, this results in the discovery of ST elevation in V2-V4 and I and aVL, diagnostic of anterolateral STEMI. The ED providers activated the cath lab, but the interventionalist refused to come in because it was "not a STEMI". The patient died 8 hours later of cardiogenicshock.
NH-IMRangiowas calculated based on standard coronary angiographic views with 3-dimensional-modeling and computational analysis of the coronary flow.RESULTS:Overall, ECC (a composite of cardiovascular death, cardiogenicshock, acute heart failure, life-threatening arrhythmias, resuscitated cardiac arrest, left ventricular thrombus, post-ST-segment–elevation (..)
It may look identical t o the ST-T wave appearance seen after a STEMI with marked troponin elevation, that has now reperfused ( be this reperfusion spontaneous — or by treatment with PCI or thrombolytics ). Unfortunately — this patient died within 12 hours of obtaining this tracing from cardiogenicshock.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck.
There is an obvious inferior STEMI, but what else? Why is the patient in shock? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. He was in profound cardiogenicshock. This STE is diagnostic of Right Ventricular STEMI (RV MI). A right sided ECG was not recorded.
Assessment was severe sudden cardiogenicshock. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 They recorded an EC G: New ST Elevation.
These were catastrophically missed (EM cath lab activation cancelled both times by the interventionalist) Here is a case of Sinus with RBBB and LAFB that was diagnosed correctly by the emergency physicians as acute STEMI. The patient died of cardiogenicshock: Go to the post to see the full explanation.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content