This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenicshock). In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonary embolism. Answer : Bedside ultrasound! So CT is required to find the diagnosis!
Background Pompe disease (PD) is a rare, progressive autosomal recessive lysosomal storage disorder that directly impacts mitochondrial function, leading to structural abnormalities and potentially culminating in heart failure or cardiogenicshock. Further genetic testing identified a homozygous mutation c.2662G>T
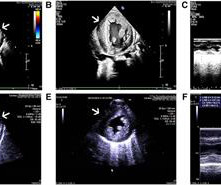
Smith comment: This patient did not have a bedside ultrasound. Had one been done, it would have shown a feature that is apparent on this ultrasound (however, this patient's LV function would not be as good as in this clip): This is recorded with the LV on the right. In fact, bedside ultrasound might even find severe aortic stenosis.
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. I would do bedside ultrasound to look at the RV, look for B lines as a cause of hypoxia (which would support OMI, and argue against PE), and if any doubt persists, a rapid CT pulmonary angiogram. There is sinus tachycardia at ~100/minute.
Case Continued 2 days later the patient became increasingly tachycardic, hypotensive, ashen, clammy (in cardiogenicshock) and had a new murmur. Rupture can be either free wall rupture (causing tamonade) or septal rupture, causing ventricular septal defect with left to right flow and resulting pulmonary edema and shock.
I have always said that tachycardia should argue against acute MI unless there is cardiogenicshock or 2 simultaneous pathologies. While sensitivity of this sign is very low — its presence is highly suggestive of longstanding and severe pulmonary disease. We showed this in a recent analysis of UTROPIA data (see abstract below).
A bedside cardiac ultrasound was normal, with no effusion. Assessment was severe sudden cardiogenicshock. and the patient was converted to veno-venous (V-V) ECMO due to persistent pulmonary insufficiency. Clinically — the patient was felt to be in cardiogenicshock. They recorded an EC G: New ST Elevation.
Whenever there is tachycardia, I am skeptical of OMI unless it has led to severely compromised ejection fracction with cardiogenicshock. I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Pulmonary edema caused by acute MI is especially worrisome.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content