This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
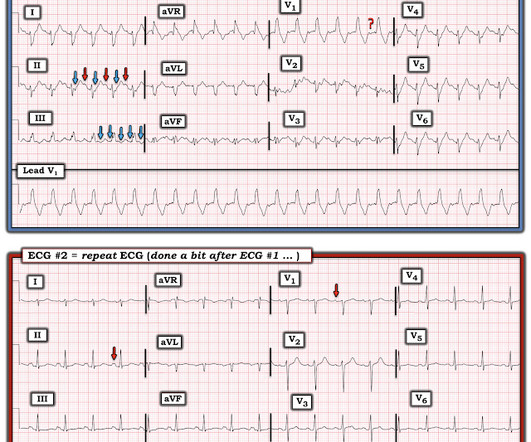
It shows sinus tachycardia with right bundle branch block. Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenicshock). In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonary embolism.
I see the following: There is sinus tachycardia ( upright P wave with fixed PR interval in lead II ) — at the rapid rate of ~130/minute. Sinus Tachycardia and RAD — as already noted above. PEARL # 2: In the absence of associated heart failure ( cardiogenicshock ) — sinus tachycardia is not a common finding in acute MI.
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. I would do bedside ultrasound to look at the RV, look for B lines as a cause of hypoxia (which would support OMI, and argue against PE), and if any doubt persists, a rapid CT pulmonary angiogram. There is sinus tachycardia at ~100/minute.
There is sinus tachycardia. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology. I have always said that tachycardia should argue against acute MI unless there is cardiogenicshock or 2 simultaneous pathologies. Here is that ECG: What do you think?
The patient was transported to the CCU for further medical optimization where a pulmonary artery catheter was placed. Authors' commentary: Cardiogenicshock in the setting of severe aortic stenosis. Fundamentally, cardiogenicshock is an issue of decreased cardiac output.
Notice I did not say "pulmonary embolism," because any form of severe acute right heart strain may produce this ECG. This includes, but is not limited to, PE, asthma/COPD exacerbation, hypoxic vasoconstriction from pneumonia, acute pulmonary hypertension exacerbation. Differences of Pulmonary Embolism T-waves from Wellens' T-waves: 1.
My answer: "This is classic for PE, but it can also be present in any hypoxia due pulmonary hypoxic vasoconstriction and resulting acute pulmonary hypertension and acute right heart strain. Tachycardia (or nearly) 2. An ECG was texted to me (Smith) without any clinical information: What did I say? This is NOT Wellens.
when the usual negative P wave deflection of sinus tachycardia is nowhere to be found in lead V1 )? While of course possible for the rhythm in ECG #1 to be either AFlutter or fascicular VT — sinus tachycardia immediately becomes a much more likely possibility once we know that this patient is critically ill with multisystem disease.
Assessment was severe sudden cardiogenicshock. and the patient was converted to veno-venous (V-V) ECMO due to persistent pulmonary insufficiency. Clinically — despite an initial 2-fold increased troponin, the normal bedside Echo was reassuring against OMI or pulmonary embolism. They recorded an EC G: New ST Elevation.
Here is another proven left main occlusion in a young woman who presented with sudden pulmonary edema, had this ECG recorded, then arrested and was resuscitated after 30 minutes of CPR: This has sinus tachycardia with RBBB and LAFB, and STE in V2-V6 as well as I, aVL This pattern could just as easily be seen in LAD occlusion.
The abnormal heart rhythms can further lead to death because of ventricular tachycardia and ventricular fibrillation. It’s essential for those at risk of coronary artery disease to be aware of the following symptoms. This indicates that restoring normal blood circulation as quickly as possible will result in less damage.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. However, there is also significant tachycardia , with heart rate of 116, and known hypoxia. She arrived to the ED with a nonrebreather mask. Her blood pressure on arrival was 153/69.
Chest X-ray also showed pulmonary edema. 1) as far as I can tell, there is very little data on amiodarone for this indication 2) amiodarone has beta blockade effects which could be deleterious in a patient with large anterior MI with pulmonary edema and at risk for cardiogenicshock (and she did go into shock.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content