This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
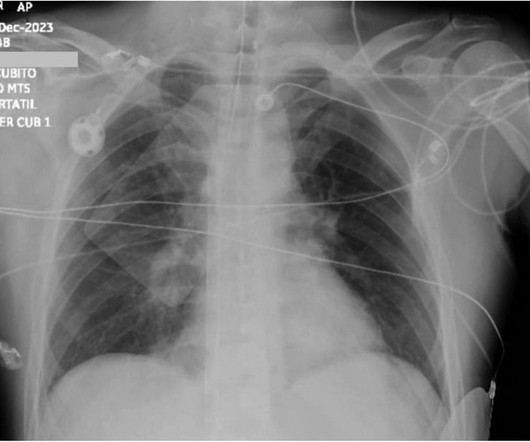
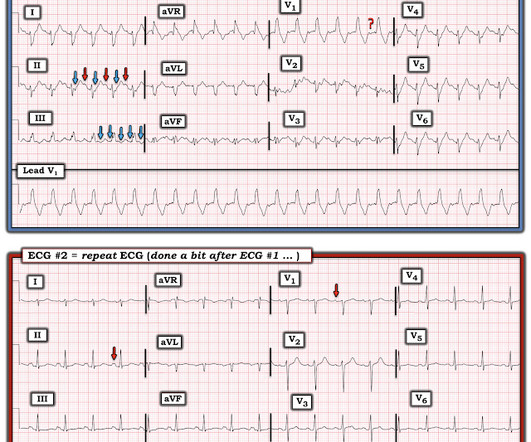
Cardiogenicshock (CS)is the most feared event following STEMI. A subset of NSTEMI precipitated by acute severe HT and flash pulmonary edema has excellent prognosis if BP is reduced promptly. Non-STEMI vs. STEMI CardiogenicShock: Clinical Profile and Long-Term Outcomes. Global ST depression (AVR.V1 Reference 1.Martínez
male, 67% acute myocardial infarction, 33% acute decompensated heart failure), 45 (41.3%), 33 (30.3%), and 31 (28.4%) were in SCAI Shock Stages C, D, and E, respectively. Patients achieving all 3 best practices significantly increased from 35.1% (P1) to 52.8% (P3) (P=0.026).
Despite the elevated mortality rates associated with high-risk pulmonary embolism (PE), this condition remains understudied. Data regarding the effectiveness and safety of invasive therapies such as venoarterial extracorporeal membrane oxygenation (VA-ECMO) in this patient population remains controversial.
Background:Venoarterial-extracorporeal membrane oxygenation (VA-ECMO) is used to treat cardiogenicshock. However, retrograde arterial perfusion from the femoral artery can increase left ventricular (LV) afterload, resulting in LV distention which may hamper myocardial recovery and worsen pulmonary congestion.
Cardiogenicshock continues to carry a high mortality rate despite contemporary care, with no breakthrough therapies shown to improve survival over the past few decades. A slowly maturing evidence base has suggested that cardiogenicshock teams may improve patient outcomes.
Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenicshock). In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonary embolism. In PE, there is almost always some hypoxia without any pulmonary edema.
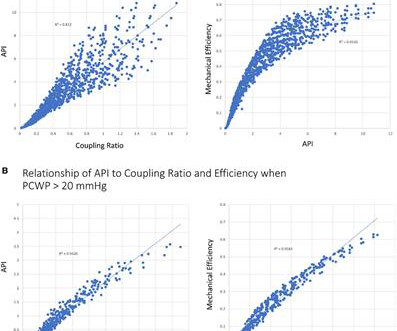
Nature Reviews Cardiology, Published online: 22 February 2024; doi:10.1038/s41569-024-01002-4 Using a porcine model of cardiogenicshock, Lamberti and colleagues develop a clinically accessible, patient-validated metric to assess pulmonary vascular compliance that can predict tolerance to left-sided ventricular assist device support.
API strongly correlated with the left ventricular coupling ratio ( R 2 = 0.81) and the strength of association became even stronger under loaded conditions where pulmonary capillary wedge pressure (PCWP) was >20 mmHg ( R 2 = 0.94). Results Approximately 1010 discrete heart failure scenarios were modeled.
BackgroundCardiogenic shock complicating acute myocardial infarction is associated with a high mortality rate. Cardiogenicshock after outofhospital cardiac arrest (OHCA) can be due to transient myocardial stunning but also reflect the increasing severity of ongoing heart failure. Of 789 patients included, 31.6%
Background Pompe disease (PD) is a rare, progressive autosomal recessive lysosomal storage disorder that directly impacts mitochondrial function, leading to structural abnormalities and potentially culminating in heart failure or cardiogenicshock. Further genetic testing identified a homozygous mutation c.2662G>T
large ASD, partial anomalous pulmonary venous return, significant tricuspid regurgitation, carcinoid valvular disease, etc,) 2) Conditions causing pressure overload of the RV. Any cause of pulmonary hypertension. There is normal axis, normal R-wave progression in the precordial leads and no intraventricular conduction abnormalities.
PEARL # 2: In the absence of associated heart failure ( cardiogenicshock ) — sinus tachycardia is not a common finding in acute MI. For a 10-minute video review on reading Pulmonary CT Scan — WATCH_this_VIDEO by Dr. Jake Gibbons. For now — Let's continue with ECG signs consistent with and suggestive of acute RV "Strain".
The patient was transported to the CCU for further medical optimization where a pulmonary artery catheter was placed. Authors' commentary: Cardiogenicshock in the setting of severe aortic stenosis. Fundamentally, cardiogenicshock is an issue of decreased cardiac output.
The patient died of cardiogenicshock: Go to the post to see the full explanation. Wide Complex Tachycardia; It's really sinus, RBBB + LAFB, and massive ST elevation This is a similar case of a 20-something year old woman, previously healthy, with acute pulmonary edema. So he would not cath the patient.
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. I would do bedside ultrasound to look at the RV, look for B lines as a cause of hypoxia (which would support OMI, and argue against PE), and if any doubt persists, a rapid CT pulmonary angiogram. There is sinus tachycardia at ~100/minute.
A 35-year-old gravida 1, para 0 with biventricular heart failure (LVEF 25%), nonischemic cardiomyopathy, history stroke, history of left ventricular thrombus, class III obesity, and chronic kidney disease who had been followed by Cardio-Obstetrics throughout her pregnancy presented at 34 weeks gestation for planned induction of labor.
Notice I did not say "pulmonary embolism," because any form of severe acute right heart strain may produce this ECG. This includes, but is not limited to, PE, asthma/COPD exacerbation, hypoxic vasoconstriction from pneumonia, acute pulmonary hypertension exacerbation. Differences of Pulmonary Embolism T-waves from Wellens' T-waves: 1.
Then the notes mention "cardiogenicshock" but without any reference to a cardiac echo or to a chest x-ray. Was there pulmonary edema? They were worried that the syncope was seizure and that she had brain mets. Then they were worried about sepsis as an etiology of hypotension. Not mentioned in physicians' notes.
I have always said that tachycardia should argue against acute MI unless there is cardiogenicshock or 2 simultaneous pathologies. While sensitivity of this sign is very low — its presence is highly suggestive of longstanding and severe pulmonary disease. We showed this in a recent analysis of UTROPIA data (see abstract below).
My answer: "This is classic for PE, but it can also be present in any hypoxia due pulmonary hypoxic vasoconstriction and resulting acute pulmonary hypertension and acute right heart strain. Tachycardia is unusual in ACS unless there is cardiogenicshock or a second simultaneous pathology. This is NOT Wellens.
Case Continued 2 days later the patient became increasingly tachycardic, hypotensive, ashen, clammy (in cardiogenicshock) and had a new murmur. Rupture can be either free wall rupture (causing tamonade) or septal rupture, causing ventricular septal defect with left to right flow and resulting pulmonary edema and shock.
Assessment was severe sudden cardiogenicshock. and the patient was converted to veno-venous (V-V) ECMO due to persistent pulmonary insufficiency. Clinically — despite an initial 2-fold increased troponin, the normal bedside Echo was reassuring against OMI or pulmonary embolism. They recorded an EC G: New ST Elevation.
Here is another proven left main occlusion in a young woman who presented with sudden pulmonary edema, had this ECG recorded, then arrested and was resuscitated after 30 minutes of CPR: This has sinus tachycardia with RBBB and LAFB, and STE in V2-V6 as well as I, aVL This pattern could just as easily be seen in LAD occlusion.
BACKGROUND:There are limited large-scale data on the outcomes of patients with cardiogenicshock (CS) transferred to hub centers. During the hospitalization, they had higher rates of renal failure, pulmonary artery catheter use, and mechanical circulatory support use. Circulation: Heart Failure, Ahead of Print.
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
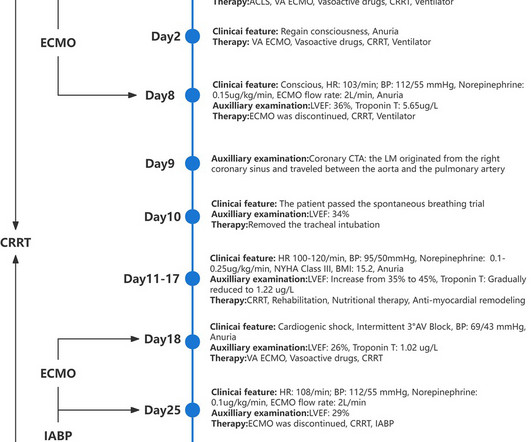
A young female patient suffered cardiogenicshock after undergoing surgery for an ectopic pregnancy. Coronary artery computed tomography angiography (CTA) revealed a left main artery (LM) originating from the right coronary sinus and traveling between the aorta and pulmonary artery.
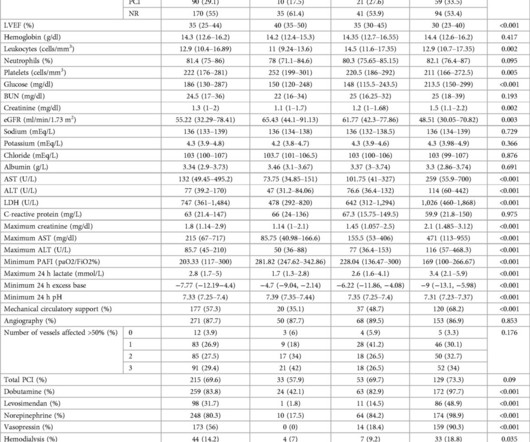
This study investigates the impact of vasoactive drug use and in-hospital outcomes among AMI-CS.Materials and methodsA total of 309 patients who underwent pulmonary artery catheterization between 2006 and 2021 were categorized by the number of vasoactive drugs used (01, 2, or >2). Clinical and 24h hemodynamic data were analyzed.
Whenever there is tachycardia, I am skeptical of OMI unless it has led to severely compromised ejection fracction with cardiogenicshock. I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Acute coronary occlusion and acute pulmonary edema can coexist.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content