This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
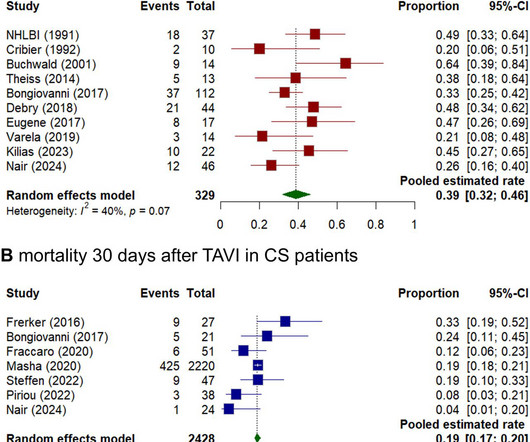
Background Cardiogenicshock (CS) induced by severe aortic stenosis (AS) is a life-threatening condition with high mortality. Despite advancements in emergency interventions, the optimal treatment approach remains uncertain. The primary endpoint was mortality at 30 days. Results Seventeen studies were included, totalling 2811 patients.
A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenicshock. She was worked as a full code, and ROSC was achieved. She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. Later the next day, she went into cardiac arrest again.
He has a pacemaker for an unknown arrhythmia reason, and has a hx of a PE but is not anti-coagulated currently. He went into cardiogenicshock and is intubated in the cardiac ICU. Modified-Smith-Sgarbossa Criteria provide objective criteria for assessing patients with LBBB and/or pacemaker tracings for acute coronary disease.
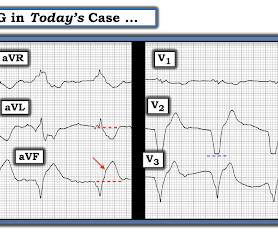
The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing").
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. It is true that assessment of pacemaker tracings for acute ST-T wave changes can be challenging. Sent by Pete McKenna M.D.
Rapid Fire Challenging Structural Heart Imaging Cases with Heart Team Panel; Follow-up of Pacemakers and ICDS for the Non-electrophysiologist; The Real Reasons Your Patient with Heart Failure was Readmitted: Noncardiac Comorbidities, Geriatric Syndromes and Social Determinants of Health; and Death by a Thousand Cuts!
These issues can only be addressed in an ICCU (Intensive Coronary Care Unit) setting, where temporary pacemakers and defibrillators are available. It’s essential for those at risk of coronary artery disease to be aware of the following symptoms.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content