This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
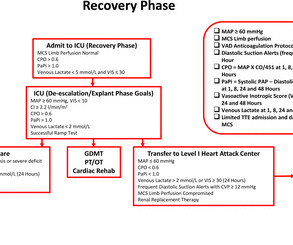
The goal of the DanGer Shock trial was to compare the safety and efficacy of Impella CP on top of standard care compared with standard care alone among patients with ST-segment elevation myocardialinfarction (STEMI) and cardiogenicshock.
Nature Reviews Cardiology, Published online: 23 April 2024; doi:10.1038/s41569-024-01035-9 Data from the DanGer Shock trial demonstrate that implantation of a microaxial flow pump in patients with ST-segment elevation myocardialinfarction complicated by cardiogenicshock increases the survival rate compared with standard care alone.
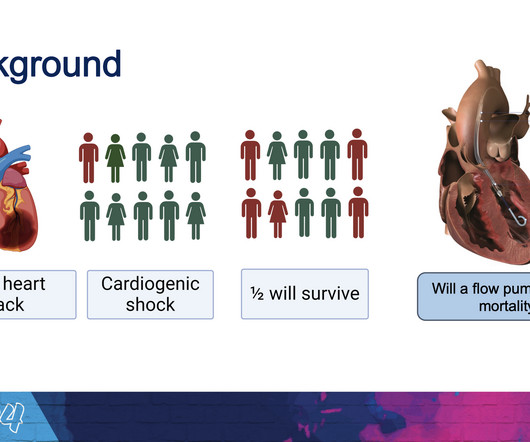
Cardiogenicshock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset How is CS in NSTEMI different ?
Introduction Cardiogenicshock (CS) complicates 5%–15% of cases of acute myocardialinfarction (AMI) with inpatient mortality greater than 40%. This prospective registry includes all patients >18 years of age presenting with STEMI with or without CS beginning on 1 February 2023.
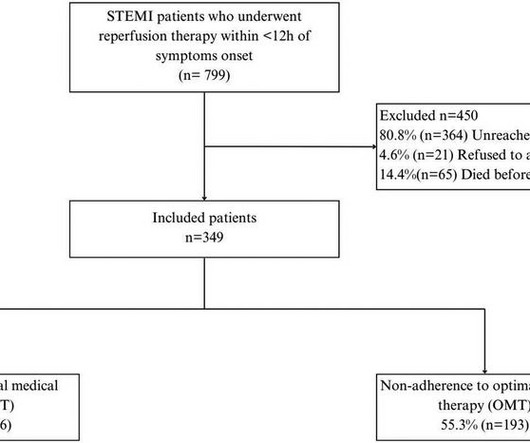
IntroductionIn developing countries, there is a notable scarcity of real-world data on adherence to optimal medical therapy (OMT) and its correlation with major cardiovascular adverse events (MACEs) after ST-elevation myocardialinfarction (STEMI). Patients were followed up for 4.5 years (±10.9), predominantly male (89.9%).
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardialinfarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). PIRP is strongly associated with myocardial rupture. The VSR is what is causing the cardiogenicshock! Heart rate was in the 80s.
Subtle as a STEMI." (i.e., A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenicshock. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. This one is easy for the Queen. 2023;82:194–202.
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
milla1cf Mon, 04/08/2024 - 18:07 April 8, 2024 — Implantation of the Impella CP micro-axial flow pump in the hours after a heart attack significantly increased the rate of survival at six months among people suffering cardiogenicshock, according to a study presented at the American College of Cardiology ’s Annual Scientific Session.
BACKGROUND:Patients with ST-segment–elevation myocardialinfarction but no coronary microvascular injury are at low risk of early cardiovascular complications (ECC). CONCLUSIONS:NH-IMRangiois a valuable risk-stratification tool in patients with ST-segment–elevation myocardialinfarction.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. He expired 4 days later.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck.
There is an obvious inferior posterior STEMI(+) OMI. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E. What is the atrial activity? Is it sinus arrest with junctional escape?
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
Clinical presentation was stable angina 130/567 (22.9%), non-ST-elevation acute coronary syndrome (NSTEACS) 312/567 (55%), ST-elevation myocardialinfarction (STEMI) 125/567 (22.0%), and STEMI with cardiogenicshock 13/125 (10.4%). and the average number of stents 2.6.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). The notes now refer to the patient being in cardiogenicshock, on pressors. Eur J Emerg Med. 2017;24:236–242.
Assessment was severe sudden cardiogenicshock. Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 What is it?
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. Authors' commentary: Cardiogenicshock in the setting of severe aortic stenosis. What do you see?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
LAD 80% mid LCx occluded mid (acute infarct lesion) RCA 80% mid. PCI mid LCx So this is an OMI (Occlusion MyocardialInfarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. The patient went into cardiogenicshock and ultimately died of this MI. distal stent patent.
There is an obvious inferior STEMI, but what else? Why is the patient in shock? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. He was in profound cardiogenicshock. This STE is diagnostic of Right Ventricular STEMI (RV MI). A right sided ECG was not recorded.
I have always said that tachycardia should argue against acute MI unless there is cardiogenicshock or 2 simultaneous pathologies. The goal of the present analysis was to examine whether the presence of tachycardia identified patients unlikely to have type 1 myocardialinfarction.
This pattern is essentially always accompanied by cardiogenicshock and high rates of VT/VF arrest, etc. The patient arrived to the ED in cardiogenicshock but awake. Code STEMI was activated. A man in his 80s with chest pain What, besides large anterior STEMI, is so ominous about this ECG? Eur Heart J.
Because of the tachcardia, I would expect her to be very poor left ventricular function and maybe Cardiogenicshock. Alternatively , it is someone who has an old myocardialinfarction and is now very sick with something else. Below is my response. There is sinus tach. There is an incomplete RBBB and LAFB. LV Aneurysm?
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenicshock" is not applicable outside of sinus rhythm. Is that an obvious STEMI underneath that rhythm? Is this inferor STEMI? Atrial Flutter with Inferior STEMI? If I fix the rhythm will the ST changes resolve?
A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al. were pretty sick, with mostly LM/pLAD lesions and high rates of cardiogenicshock. I had no idea SCAD was so common a cause of acute STEMI in younger women, even when they are non-smokers.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content