This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
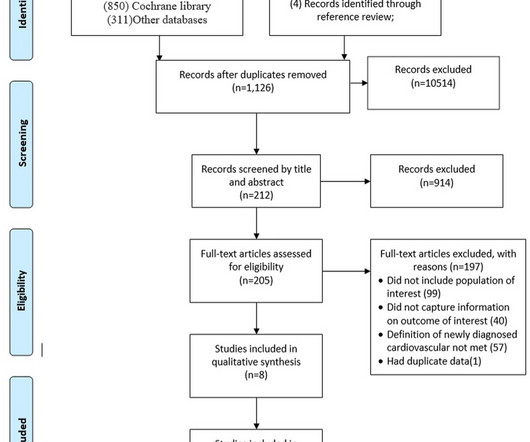
Care for survivors after an acute attack of COVID-19 should include paying close attention to cardiovascular health and disease.Systematic Review RegistrationPROSPERO [CRD42022353965].
BackgroundClinical outcome of ischemic cardiogenicshock (CS) requiring extracorporeal membrane oxygenation is highly variable, necessitating appropriate assessment of prognosis. However, a systemic predictive model estimating the mortality of refractory ischemic CS is lacking. Among 322 patients, 138 (42.9%) survived postdischarge.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. Figure B At this point, with the ECG changing from diffuse ST depression to widespread ST elevation and the patient presenting in cardiogenicshock, left main coronary artery (LMCA) occlusion is the likely diagnosis.
Abstract Objectives This study aimed to assess the impact of anemia and iron deficiency (ID) on clinical outcome in patients with cardiogenicshock (CS) complicating acute myocardial infarction (AMI).
The VSR is what is causing the cardiogenicshock! Mechanical complications occur acutely and significantly alter hemodynamics leading to comp ensatory mechanism which usually involve vasoconstriction and tachycardia, both hallmarks of cardiogenicshock. PIRP is strongly associated with myocardial rupture.
Written by Willy Frick with edits by Ken Grauer A woman in her 70s with a history of hypertension presented with acute onset shortness of breath. Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenicshock). Her ECG is shown below: What do you think?
Impella Left Sided Blood Pumps also are used when there is ongoing cardiogenicshock that occurs less than 48 hours after a severe heart attack (acute myocardial infarction), open-heart surgery, or when the heart is not functioning well due to a condition called cardiomyopathy.
years to monitor MACEs (cardiovascular death, cardiogenicshock, recurrent myocardial infarction, and heart failure).ResultsWe Hypertension (42.4%), smoking (34.3%), type 2 diabetes mellitus (31.2%), obesity (22.92%), and dyslipidemia (21.4%) were highly prevalent. Patients were followed up for 4.5
PMR patients had fewer cardiovascular risk factors: hypertension (52% vs. 73%, p =0.04), diabetes (26% vs. 48%, p <0.01) but a higher left ventricular ejection fraction (4515% vs.3510%, p <0.01) compared secondary MR patients. Aetiology of MR, cardiogenicshock, and procedure timing significantly impacted in-hospital mortality.
Background There is increasing awareness that patients without standard modifiable risk factors (SMuRFs; diabetes, hypercholesterolaemia, hypertension and smoking) may represent a unique subset of patients with acute coronary syndrome (ACS). vs 50.8%, p<0.001) and were more likely to experience postprocedural cardiogenicshock (4.5%
Propensity score-matched analysis (PSM) (1:1) was performed on age, gender, BMI, hypertension, diabetes mellitus, chronic kidney disease, hemoglobin level, LDL level, left ventricular ejection fraction and various drugs including beta blockers, ACEi and ARBi. 0.89), P<0.001), and after 1 year (RR, 0.91 (95% CI: 0.86-0.96),
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. Authors' commentary: Cardiogenicshock in the setting of severe aortic stenosis. Fundamentally, cardiogenicshock is an issue of decreased cardiac output.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The notes now refer to the patient being in cardiogenicshock, on pressors.
ET Main Tent (Hall B1) Effect of Gamification, Financial Incentives or Both Combined to Increase Physical Activity Among Patients with Elevated Risk For Major Adverse Cardiovascular Events.
Any cause of pulmonary hypertension. large ASD, partial anomalous pulmonary venous return, significant tricuspid regurgitation, carcinoid valvular disease, etc,) 2) Conditions causing pressure overload of the RV. Smith's book : Learning points: 1) OMI can be very subtle and RV infarction may manifest poorly on the standard ECG.
Case submitted and written by Dr. Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chest pain and collapsed, and had bystander CPR. But by this time the patient went into cardiogenicshock and passed away.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergency department for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. Here is his triage ECG which was obtained at 20:34 during active pain.
Past medical history included diabetes and hypertension. As often emphasized by Dr. Smith — sinus tachycardia is not a common finding with acute OMI unless something else is going on (ie, cardiogenicshock ). CT chest showed left sided pulmonary embolism and a pulmonary infarct that had previously been mistaken for pneumonia.
Assessment was severe sudden cardiogenicshock. Higher troponin correlated with more history of heart failure, diabetes, and hypertension, as well as higher D-dimer, and nearly all inflammatory markers. Clinically — the patient was felt to be in cardiogenicshock. They recorded an EC G: New ST Elevation.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Interestingly, this patient was seen in the ED for hypertension and headache 3 days earlier. Sent by Pete McKenna M.D.
He had history of prior MIs and CABG, as well as diabetes, hypertension, and hyperlipidemia. He was in cardiogenicshock requiring an impella for several days after cath. The pain was still ongoing at arrival. He also noted a bilateral "odd feeling" in his arms. He stated it was similar to prior heart attacks.
Tortuous LAD consistent with hypertensive cardiac disease and luminal irregularities, but free of stenosis 3. Had such been the case, this patient would likely have been a prehospital cardiac arrest, or have been in profound cardiogenicshock at the time of ED arrival. Distal LM stenosis (80%), not acutely thrombosed b.
This includes, but is not limited to, PE, asthma/COPD exacerbation, hypoxic vasoconstriction from pneumonia, acute pulmonary hypertension exacerbation. When there is tachycardia, the patient is in cardiogenicshock with very poor LV function on bedside echo. The T-waves simply look different in Wellens'.
My answer: "This is classic for PE, but it can also be present in any hypoxia due pulmonary hypoxic vasoconstriction and resulting acute pulmonary hypertension and acute right heart strain. Tachycardia is unusual in ACS unless there is cardiogenicshock or a second simultaneous pathology. This is NOT Wellens. The answer was yes.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. BP was 110 and oxygen saturation was normal.
He was hypertensive and tachycardic, with mildly increased work of breathing. The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenicshock" is not applicable outside of sinus rhythm. Here is his initial ECG: What do you think? What will you do for this patient?
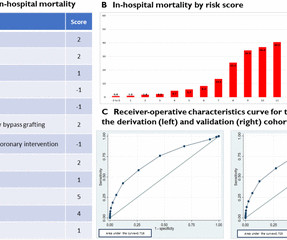
A novel risk score was developed, including the following parameters: male sex, age >70 years, non-white race, hypertension, hyperlipidemia, history of coronary artery bypass grafting, history of percutaneous coronary intervention, cardiac arrhythmias, renal failure, cardiogenicshock and vasopressor use.
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The Society (..)
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chest pain and shortness of breath. Whenever there is tachycardia, I am skeptical of OMI unless it has led to severely compromised ejection fracction with cardiogenicshock. This was written by Hans Helseth.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content