This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenicshock. So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? This was sent by a reader. and K was normal. Here was the ECG: There is sinus tachycardia.
She presented to an outside hospital after several days of malaise and feeling unwell. The VSR is what is causing the cardiogenicshock! It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI.
milla1cf Mon, 04/08/2024 - 18:07 April 8, 2024 — Implantation of the Impella CP micro-axial flow pump in the hours after a heart attack significantly increased the rate of survival at six months among people suffering cardiogenicshock, according to a study presented at the American College of Cardiology ’s Annual Scientific Session.
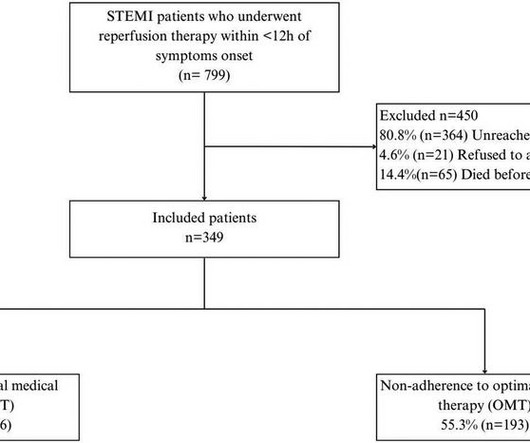
IntroductionIn developing countries, there is a notable scarcity of real-world data on adherence to optimal medical therapy (OMT) and its correlation with major cardiovascular adverse events (MACEs) after ST-elevation myocardial infarction (STEMI). Patients were followed up for 4.5 ResultsWe included 349 patients with a mean age of 58.08
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. The patient was extubated on Day-3 of the hospital stay. The below ECG was recorded.
Discharging patients with NH-IMRangio<40 units at 48 hours after admission would reduce the total in-hospital stay by 943 days (median 2 [1–4] days per patient).CONCLUSIONS:NH-IMRangiois NH-IMRangioguided strategies to early discharge may contribute to safely shorten hospital stay, optimizing resources utilization.
It may look identical t o the ST-T wave appearance seen after a STEMI with marked troponin elevation, that has now reperfused ( be this reperfusion spontaneous — or by treatment with PCI or thrombolytics ). The remaining 13/26 patients developed these changes within 24 hours after hospital admission.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. The patient had a protracted hospitalization and did not survive.
Post-procedural data included average length of in-hospital stay, intra-hospital morbidity and mortality, and mortality or admission with ACS 12–36 months after the index procedure. A total of 567 patients underwent coronary catheterisation for the three-year period between January 2018 and December 2020.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58). What do you see?
There is an obvious inferior STEMI, but what else? Why is the patient in shock? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. He was in profound cardiogenicshock. This STE is diagnostic of Right Ventricular STEMI (RV MI). A right sided ECG was not recorded.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
This pattern is essentially always accompanied by cardiogenicshock and high rates of VT/VF arrest, etc. The patient arrived to the ED in cardiogenicshock but awake. Code STEMI was activated. A man in his 80s with chest pain What, besides large anterior STEMI, is so ominous about this ECG?
Assessment was severe sudden cardiogenicshock. 3 studied 416 patients hospitalized with COVID in China, of whom 82 had an initial cTn(I) above the upper reference limit. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease.
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. But by this time the patient went into cardiogenicshock and passed away.
PCI mid LCx So this is an OMI (Occlusion Myocardial Infarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. The patient went into cardiogenicshock and ultimately died of this MI. Setting Secondary and tertiary care hospitals in the United Kingdom and United States. Sandoval Y.
Whenever there is tachycardia, I am skeptical of OMI unless it has led to severely compromised ejection fracction with cardiogenicshock. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Truly, the Marquette 12 SL algorithm correctly identifies this STEMI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content