This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A summary of current and novel biomarkers and their potential stages of release in cardiogenicshock. The diagram illustrates the proposed release of the biomarkers during the different stages of cardiogenicshock: progression from cardiac dysfunction/stress, through to inflammation and end-organ dysfunction.
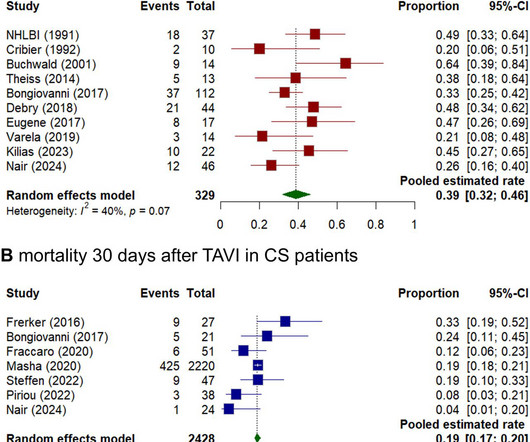
Background Cardiogenicshock (CS) induced by severe aortic stenosis (AS) is a life-threatening condition with high mortality. In-hospital mortality pooled estimated rates were 11% for eTAVI (CI 0.06 - 0.18) and for eBAV 40% (CI 0.28 - 0.54). Methods A systematic literature review and meta-analysis was performed.
A simplified risk stratification model based on the cardiogenicshock (CS) classification system from the Society for Cardiovascular Angiography and Intervention (SCAI) effectively predicts in-hospital mortality in postcardiotomy (PC) patients, according to a retrospective, observational study.
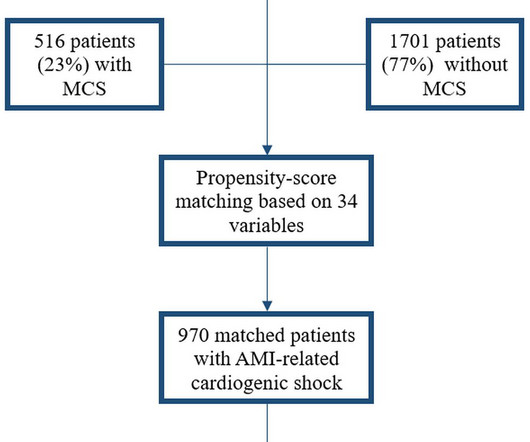
Background Despite limited beneficial evidence, mechanical circulatory support (MCS) is commonly used in patients with acute myocardial infarction-related cardiogenicshock (AMI-CS). In this Dutch registry, we investigated MCS usage, associated patient characteristics and clinical outcomes.
Published results of a large, national heart attack study show that patients with a life-threatening complication known as cardiogenicshock survived at a significantly higher rate when treated with a protocol developed by cardiologists at Henry Ford Health, in collaboration with 80 hospitals nationwide.
Windtree Therapeutics’ istaroxime appears to have scored in its latest Phase 2b trial , showing that the steroidal drug significantly improves systolic blood pressure in cardiogenicshock patients. That could be a big deal in the cardiogenicshock space, which many believe is still in need of more effective treatments.
Cardiogenicshock continues to portend poor outcomes, conferring short-term mortality rates of 30% to 50% despite recent scientific advances. Age is a nonmodifiable risk factor for mortality in patients with cardiogenicshock and is often considered in the decision-making process for eligibility for various therapies.
Advances in critical care therapies for patients with cardiogenicshock (CS), including temporary mechanical circulatory support and multidisciplinary shock teams, have led to improved survival to hospital discharge, ranging from 60% to 70%. Circulation, Volume 151, Issue 3 , Page 257-271, January 21, 2025.
A 55-year-old man had an out-of-hospital cardiac arrest. An evaluation showed 2-mm ST-segment elevations in the inferior leads on electrocardiography, cardiogenicshock, and a new systolic murmur. A diagnosis was made.
A 20-something presented after a huge verapamil overdose in cardiogenicshock. Today's patient is a young male who presented in cardiogenicshock following a massive verapamil overdose. He had been seen at an outside institution and been given 6 g calcium gluconate, KCl, and a norepinephrine drip. The initial K was 3.0
Publication date: Available online 24 January 2025 Source: The American Journal of Cardiology Author(s): Eric J. Hall, Colby R. Ayers, Nicholas S. Hendren, Christopher Clark, Amit Saha, Hadi Beaini, Isabella L. Alexander, Evan P. Gee, Ian R. McConnell, Emily S. Samson, Roslyn J. Saplicki, Christopher S. Grubb, Grant Tucker, Justin L.
Baylor Scott & White The Heart Hospital-Plano in Texas cut times of cardiogenicshock diagnosis in half after implementing a quality improvement project that included nurse education and an electronic shock team alert, according to a study published Dec. 1 in Critical Care Nurse.
BackgroundVenoarterial extracorporeal membrane oxygenation (VA‐ECMO) is increasingly used for patients with cardiogenicshock. In‐hospital mortality was higher with ECMO with Impella (54.8%) compared with ECMO only (50.4%) and ECMO with IABP (48.4%). P=0.002), higher in‐hospital mortality (aOR, 1.32;P=0.001),
with SmartAssist and Impella CP with SmartAssist heart pumps, granting premarket approval (PMA) for use in specific pediatric patients with symptomatic acute decompensated heart failure (ADHF) and cardiogenicshock. and Impella CP, both left-sided heart pumps, for pediatric patients with symptomatic ADHF and cardiogenicshock.
A nationwide observational analysis of patients with aortic stenosis (AS) and cardiogenicshock (CS) who underwent transcatheter aortic valve replacement (TAVR) or surgical aortic valve replacement (SAVR) determined that patients who underwent TAVR had lower in-hospital complications and resource utilization compared with SAVR.
A cardiovascular specialty hospital in north Texas decreased time to diagnosis for patients with cardiogenicshock by more than half, according to a study published in Critical Care Nurse.
In a seminal case series published in 1967, Killip and Kimball reported 81% in-hospital mortality for patients presenting with acute myocardial infarction complicated by cardiogenicshock (AMI-CS).
BackgroundAcute myocardial infarction complicated by cardiogenicshock (AMI‐CS) is associated with significant morbidity and mortality. The primary end point was in‐hospital mortality. Survival rates to hospital discharge were high. A total of 406 patients were enrolled at 80 sites between 2016 and 2020.
Despite initiating thrombolysis for cerebral infarction and supportive treatments for heart failure, including VA-ECMO, the patient's condition continued to decline, evidenced by cardiogenicshock, heart failure, and progressive neurological deficits including coma and dilated non-reactive pupils.
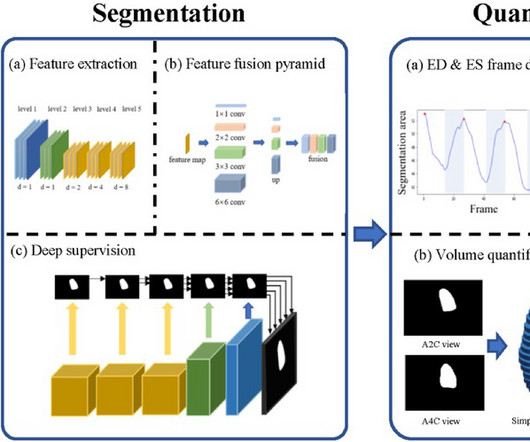
BackgroundPercutaneous extracorporeal membrane oxygenation (ECMO) is administered to pediatric patients with cardiogenicshock or cardiac arrest. The traditional method uses focal echocardiography to complete the left ventricular measurement.
A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenicshock. Referring to Figure-1 — this 53-year old woman who presented in extremis with cardiogenicshock and an initial pH = 6.9, This was sent by a reader. and K was normal. Here was the ECG: There is sinus tachycardia.
Impella and venoarterial extracorporeal membrane oxygenation (VA-ECMO) in patients with acute myocardial infarction-related cardiogenicshock (AMICS). Impella patients were older (34% vs. 13% >75 years, p < 0.001) and less frequently presented after an out-of-hospital cardiac arrest (18% vs. 40%, p < 0.001).
Abstract Worldwide, valvular heart disease (VHD) is a common cause of hospitalization for acute heart failure. In acute heart failure caused by VHD, symptoms result from rapid haemodynamic changes and subsequent decline in cardiac function, and if left untreated, leads to acute decompensation and cardiogenicshock.
After adjusting for the confounders, the risk difference in the fourth quarter of 2021 relative to the first quarter of 2019 for in‐hospital mortality was not significant (adjusted odds ratio, 0.84 [95% CI, 0.69–1.01]).ConclusionsOur Journal of the American Heart Association, Volume 12, Issue 23 , December 5, 2023.
FDA for two clinical indications: high-risk percutaneous coronary intervention (HR-PCI) and cardiogenicshock (CS). The results were presented at the 2023 Transcatheter Cardiovascular Therapeutics (TCT) conference in San Francisco by Dr. Perwaiz Meraj of North Shore University Hospital. Magenta completed a U.S.
She presented to an outside hospital after several days of malaise and feeling unwell. The VSR is what is causing the cardiogenicshock! Application to Today's Case: Today's patient developed ventricular septal rupture the evening after she was admitted to the hospital. Heart rate was in the 80s.
Publication date: Available online 5 April 2024 Source: The American Journal of Cardiology Author(s): Amit Saha, Shuang Li, James A. de Lemos, Ambarish Pandey, Deepak L. Bhatt, Gregg C. Fonarow, Brahmajee K. Nallamothu, Tracy Y.MHS WangMSc, Ann Marie Navar, Eric Peterson, Roland A. Matsouaka, Anthony A. Bavry, Sandeep R. Das, Justin L.
Introduction The use of venoarterial extracorporeal membrane oxygenation (VA-ECMO) in extracorporeal cardiopulmonary resuscitation (ECPR) in selected patients after out-of-hospital cardiac arrest (OHCA) is an established method if return of spontaneous circulation cannot be achieved.
BackgroundCardiogenic shock complicating acute myocardial infarction is associated with a high mortality rate. Cardiogenicshock after outofhospital cardiac arrest (OHCA) can be due to transient myocardial stunning but also reflect the increasing severity of ongoing heart failure.
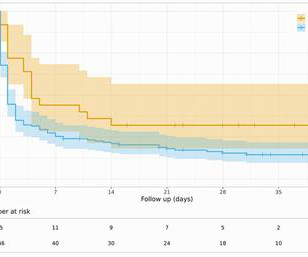
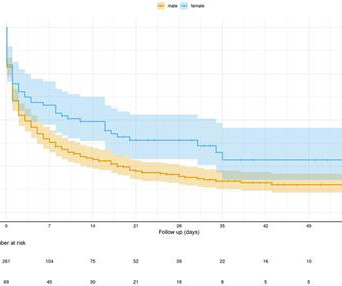
We evaluated the prognostic influence of gender in patients presenting with out-of-hospital cardiac arrest (OHCA) treated with eCPR. The primary outcome was defined as the survival of patients until they were discharged from the hospital, with a favourable neurological outcome [cerebral performance category (CPC) score of ≤2].
PMR patients were more likely to present in cardiogenicshock (91% vs. 51%, p =0.001), require mechanical circulatory support (74% vs. 34%, p =0.01), and had a higher EuroSCORE II (2313% vs. 1311%, p =0.011). Aetiology of MR, cardiogenicshock, and procedure timing significantly impacted in-hospital mortality.
New VAs during AHF have previously identified patients with higher in-hospital and 60-day morbidity and mortality. The characteristics and logistics of pre-hospital emergency medicine, as well as the density of centres capable of treating AHF and VAs, differ massively throughout Europe.
Multivariate logistic and linear regression analyses were performed, adjusting for multiple patient and hospital confounders. There was a non-significant increased risk of cardiogenicshock (aOR 1.14, 95% CI 0.87 - 1.5, Opioid use was also associated with longer hospital stay (adjusted MD [aMD] 1.07
A secondary analysis evaluated outcomes for severe HF hospitalizations (cardiogenicshock, cardiac arrest, and mechanical ventilation). Centers performing at least 1 heart transplant or left ventricular assist device were classified as ATCs. of centers), 525 037 (18.3%) were admissions to ATCs (5.5%
Secondary outcomes included in-hospital and 30-day events. vs 50.8%, p<0.001) and were more likely to experience postprocedural cardiogenicshock (4.5% Methods We analysed data from the Melbourne Interventional Group PCI Registry. Patients with coronary artery disease were excluded. The primary outcome was 30-day mortality.
Post-procedural data included average length of in-hospital stay, intra-hospital morbidity and mortality, and mortality or admission with ACS 12–36 months after the index procedure. A total of 567 patients underwent coronary catheterisation for the three-year period between January 2018 and December 2020.
This analysis included 17 843 admissions across 34 sites and compared interhospital tertiles of CCRx (eg, mechanical ventilation, mechanical circulatory support, continuous renal replacement therapy) utilization and its adjusted association with in-hospital survival using logistic regression.
Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58). Authors' commentary: Cardiogenicshock in the setting of severe aortic stenosis. Fundamentally, cardiogenicshock is an issue of decreased cardiac output.
For the sickest of cardiac patients, those who are leaving the hospital with advanced heart failure or who just had a heart attack, Virtual-First cardiology enables frequent virtual visits driven by AI-driven algorithms which identify the most pressing risks.
But the lack of traditional Sgarbossa criteria is not reassuring enough for such high pretest probability (elderly patient with chest pain, out of hospital cardiac arrest and LBBB), and the Modified Sgarbossa Criteria confirms Occlusion MI in this case. But by this time the patient went into cardiogenicshock and passed away.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content