This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
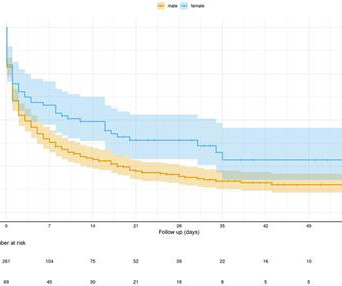
Despite the elevated mortality rates associated with high-risk pulmonaryembolism (PE), this condition remains understudied. Data regarding the effectiveness and safety of invasive therapies such as venoarterial extracorporeal membrane oxygenation (VA-ECMO) in this patient population remains controversial.
Cardiogenicshock continues to carry a high mortality rate despite contemporary care, with no breakthrough therapies shown to improve survival over the past few decades. A slowly maturing evidence base has suggested that cardiogenicshock teams may improve patient outcomes.
Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenicshock). In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonaryembolism. In PE, there is almost always some hypoxia without any pulmonary edema.
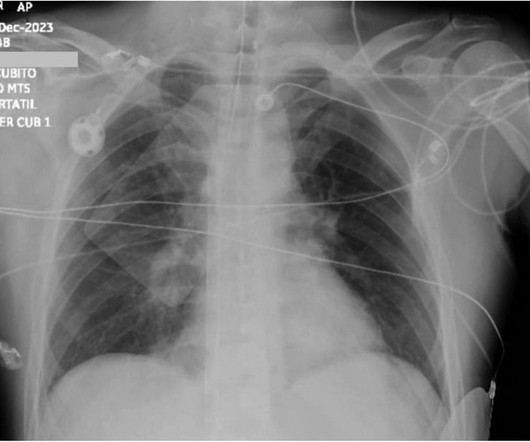
Smith comment: before reading anything else, this case screamed pulmonaryembolism to me. I would do bedside ultrasound to look at the RV, look for B lines as a cause of hypoxia (which would support OMI, and argue against PE), and if any doubt persists, a rapid CT pulmonary angiogram. There is sinus tachycardia at ~100/minute.
Notice I did not say "pulmonaryembolism," because any form of severe acute right heart strain may produce this ECG. This includes, but is not limited to, PE, asthma/COPD exacerbation, hypoxic vasoconstriction from pneumonia, acute pulmonary hypertension exacerbation. There are filling defects in both main pulmonary arteries.
My answer: "This is classic for PE, but it can also be present in any hypoxia due pulmonary hypoxic vasoconstriction and resulting acute pulmonary hypertension and acute right heart strain. Tachycardia is unusual in ACS unless there is cardiogenicshock or a second simultaneous pathology. This is NOT Wellens.
Assessment was severe sudden cardiogenicshock. and the patient was converted to veno-venous (V-V) ECMO due to persistent pulmonary insufficiency. Clinically — despite an initial 2-fold increased troponin, the normal bedside Echo was reassuring against OMI or pulmonaryembolism. What is it? There is STE in V2-V6.
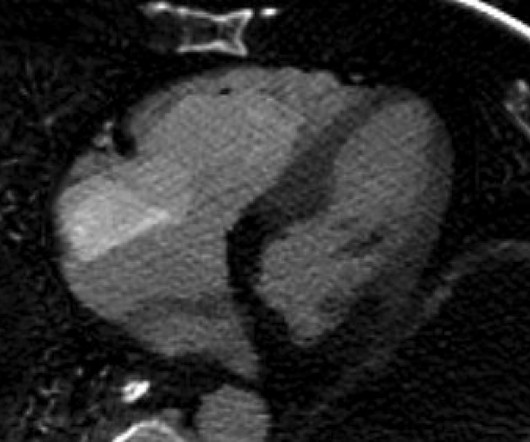
It did not show pulmonaryembolism or intra-abdominal pathology, but it did show this: See the dark area at the bottom of the image? Assessment : Cardiology thought this was cardiogenicshock from RV dysfunction. There was no pulmonaryembolism. Decreased right ventricular systolic performance.
Chest X-ray also showed pulmonary edema. LAD: type III-IV vessel with a proximal thrombotic or embolic occlusion (TIMI 0 flow). Primary VF in this study refers to fibrillation occurring in the absence of shock or pulmonary edema. She was given 2 mg Magnesium. Potassium was 4.5 She had no further episodes of VF.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content