This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
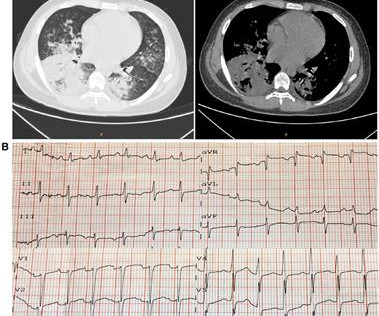
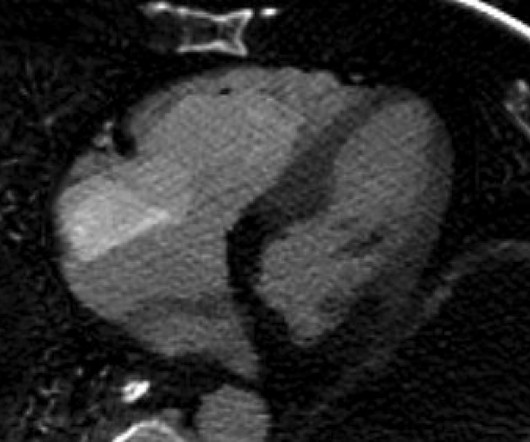
We present a case of a 15-year-old male who developed fulminant myocarditis, cardiogenicshock, and cardiac electrical storm attributed to M. pneumoniae infection. Following comprehensive treatment and rehabilitation, he was discharged in stable condition.
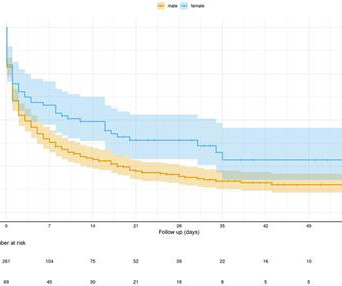
Despite the elevated mortality rates associated with high-risk pulmonary embolism (PE), this condition remains understudied. Data regarding the effectiveness and safety of invasive therapies such as venoarterial extracorporeal membrane oxygenation (VA-ECMO) in this patient population remains controversial.
Common embolism sites include the brain, spleen, kidneys, lungs, and intestines. Cardiogenicshock (CGS) is often more likely to occur after AHF has taken place. Patients with IE can experience simple CGS, septic shock, or a combination of the two.
Cardiogenicshock continues to carry a high mortality rate despite contemporary care, with no breakthrough therapies shown to improve survival over the past few decades. A slowly maturing evidence base has suggested that cardiogenicshock teams may improve patient outcomes.
Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenicshock). In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonary embolism. Additionally, there is borderline right axis deviation. Both were wrong.
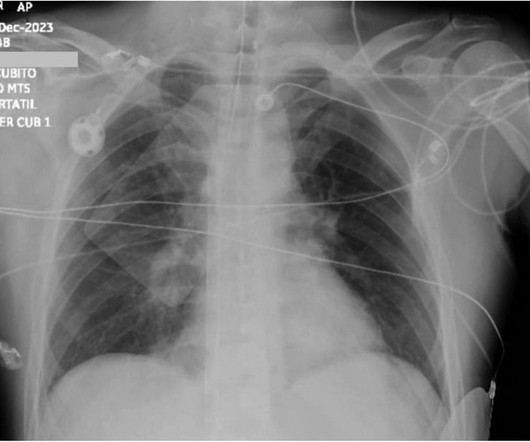
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. CT chest showed left sided pulmonary embolism and a pulmonary infarct that had previously been mistaken for pneumonia. Instead, he was diagnosed with pneumonia — that turned out to be a left-sided pulmonary embolism that was initially missed.
ET Main Tent (Hall B1) Self-expanding Versus Balloon-expandable Transcatheter Aortic Valve Replacement in Patients with Small Aortic Annuli: Primary Outcomes from the Randomized Smart Trial Effect of Edetate Disodium Based Chelation Infusions on Cardiovascular Events in Post-MI Patients with Diabetes: The TACT2 Trial Long-term Beta-blocker Treatment (..)
Notice I did not say "pulmonary embolism," because any form of severe acute right heart strain may produce this ECG. Differences of Pulmonary Embolism T-waves from Wellens' T-waves: 1. When there is tachycardia, the patient is in cardiogenicshock with very poor LV function on bedside echo. What is the answer?
No definite evidence of RV hypertrophy (normal axis, no large R-wave in V1) Late transition typical of COPD (R/S = 1 in V5) No evidence of old MI (no QS-waves in V1-V3, as seen in the presenting ECG) Other similar cases of acute right heart strain See this case of asthma whose ECG mimics acute PE: Is it pulmonary embolism? Kosuge et al.
Assessment was severe sudden cardiogenicshock. Clinically — despite an initial 2-fold increased troponin, the normal bedside Echo was reassuring against OMI or pulmonary embolism. Clinically — the patient was felt to be in cardiogenicshock. They recorded an EC G: New ST Elevation. What is it?
Tachycardia is unusual for OMI, unless the patient is in cardiogenicshock (or getting close). Then, part of the thrombus embolized into the LCx causing an inferoposterolateral OMI. (As The ECG has a lot of artifact, and the amplitude is very small, making interpretation challenging.
It did not show pulmonary embolism or intra-abdominal pathology, but it did show this: See the dark area at the bottom of the image? Assessment : Cardiology thought this was cardiogenicshock from RV dysfunction. Smith Comment: the RV was very ischemic on the CT scan and dysfunctional on echo, and this does explain the shock.
And it is definitely possible that a more proximal LCx lesion ruptured and produced distal embolism. A 2017 trial named CULPRIT SHOCK found that in patients with cardiogenicshock, a strategy of culprit vessel PCI only was associated with better outcomes than immediate multivessel PCI.
LAD: type III-IV vessel with a proximal thrombotic or embolic occlusion (TIMI 0 flow). The patient was transported to cath lab accompanied by the resident, with BP 50/30 en route improved with a push dose of 100 mcg epi. She had no further episodes of VF. Angiogram: 2. The final angiographic result is very good.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content