This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She presented to an outside hospital after several days of malaise and feeling unwell. The VSR is what is causing the cardiogenicshock! Application to Today's Case: Today's patient developed ventricular septal rupture the evening after she was admitted to the hospital. Heart rate was in the 80s.
PMR patients had fewer cardiovascular risk factors: hypertension (52% vs. 73%, p =0.04), diabetes (26% vs. 48%, p <0.01) but a higher left ventricular ejection fraction (4515% vs.3510%, p <0.01) compared secondary MR patients. Aetiology of MR, cardiogenicshock, and procedure timing significantly impacted in-hospital mortality.
Background There is increasing awareness that patients without standard modifiable risk factors (SMuRFs; diabetes, hypercholesterolaemia, hypertension and smoking) may represent a unique subset of patients with acute coronary syndrome (ACS). Secondary outcomes included in-hospital and 30-day events. vs 9.9%, p=0.029).
Post-procedural data included average length of in-hospital stay, intra-hospital morbidity and mortality, and mortality or admission with ACS 12–36 months after the index procedure. A total of 567 patients underwent coronary catheterisation for the three-year period between January 2018 and December 2020.
Past medical history included diabetes and hypertension. The patient had a protracted hospitalization and did not survive. As often emphasized by Dr. Smith — sinus tachycardia is not a common finding with acute OMI unless something else is going on (ie, cardiogenicshock ). Vitals were normal.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. BP was 110 and oxygen saturation was normal.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. Figure B At this point, with the ECG changing from diffuse ST depression to widespread ST elevation and the patient presenting in cardiogenicshock, left main coronary artery (LMCA) occlusion is the likely diagnosis.
Abstract Objectives This study aimed to assess the impact of anemia and iron deficiency (ID) on clinical outcome in patients with cardiogenicshock (CS) complicating acute myocardial infarction (AMI). ID has no relevant impact on clinical outcome in patients with CS.
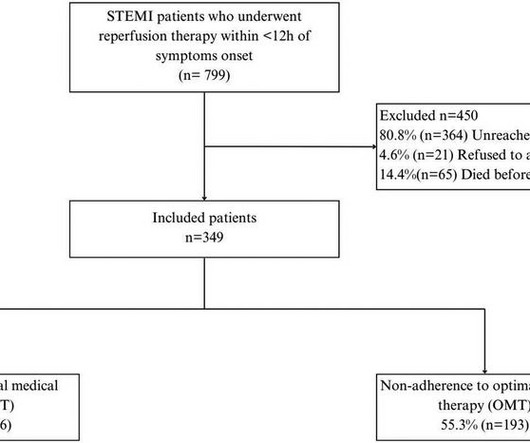
Our study focuses on addressing this gap by evaluating adherence to OMT, examining its influence on the risk of MACEs after STEMI, and assessing subsequent cardiovascular risk factor control in Mexico.MethodsWe conducted a prospective observational study of post-STEMI patients after hospital discharge. Patients were followed up for 4.5
Assessment was severe sudden cardiogenicshock. 3 studied 416 patients hospitalized with COVID in China, of whom 82 had an initial cTn(I) above the upper reference limit. Higher troponin correlated with more history of heart failure, diabetes, and hypertension, as well as higher D-dimer, and nearly all inflammatory markers.
Mark Erfe Outcomes of Sutureless/Rapid Deployment Valves Compared to Traditional Bioprosthetic Aortic Valves The Annals of Thoracic Surgery September 2020 J.
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
However, recent studies have observed that people below 40 are also experiencing heart attacks due to high blood pressure, cholesterol, diabetes, smoking, obesity, a sedentary lifestyle, and social and mental stress. Suppose there is a delay in reaching a cardiac cath-lab-equipped hospital. So, how do you recognize a heart attack?
24) Microaxial Flow Pump in Infarct-Related CardiogenicShock DanGer Shock (ACC.24) 24 and TCT 2024) Colchicine in AMI CLEAR SYNERGY (OASIS 9) (TCT 2024 and AHA 2024) Semaglutide Treatment Effect in People With Obesity and HFpEF and Diabetes Mellitus STEP-HFpEF DM (ACC.24)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content