This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration. His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. Further information is not available.
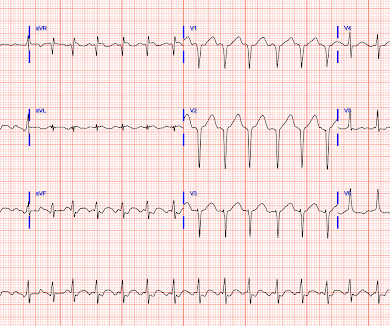
Figure B At this point, with the ECG changing from diffuse ST depression to widespread ST elevation and the patient presenting in cardiogenicshock, left main coronary artery (LMCA) occlusion is the likely diagnosis. The arrhythmia spontaneously converted before defibrillation was achieved. This is an ominous sign. As per Dr.
The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation.
Risk stratification and criteria/best time point for coronary intervention and implantable cardioverter-defibrillator implantation, however, are still controversial topics in this difficult clinical setting. New VAs during AHF have previously identified patients with higher in-hospital and 60-day morbidity and mortality.
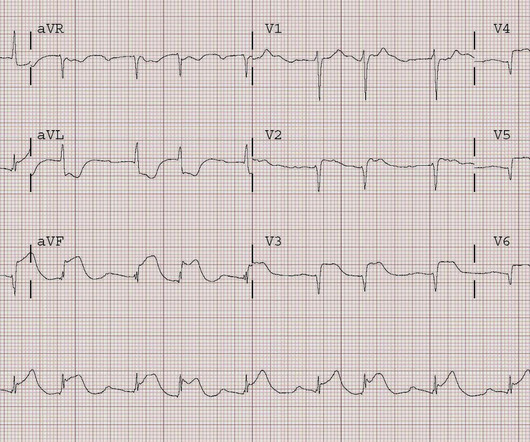
She was defibrillated successfully from ventricular fibrillation and developed a perfusing rhythm. She arrived comatose and in cardiogenicshock and the following ECG was recorded. A 56 yo f with h/o HTN and hypercholesterolemia called EMS from home after onset of L chest pain radiating to the left arm. She was intubated.
The patient is started on epinephrine infusion for cardiogenicshock and cardiology took the patient to the cath lab. During angiogram in the cath lab, the patient suffered two episodes of ventricular fibrillation for which he was successfully defibrillated.
Tachycardia is unusual for OMI, unless the patient is in cardiogenicshock (or getting close). Rhythm C: This telemetry strip from an older adult was initially thought to need defibrillation. The ECG has a lot of artifact, and the amplitude is very small, making interpretation challenging.
These issues can only be addressed in an ICCU (Intensive Coronary Care Unit) setting, where temporary pacemakers and defibrillators are available. It’s essential for those at risk of coronary artery disease to be aware of the following symptoms.
Abstract Aims Left ventricular unloading by percutaneous microaxial flow-pump devices has been shown to improve survival in patients with cardiogenicshock (CS). Summary of key study outcomes. The objective of the study is to examine whether Impella 5.0/5.5
In the second case, the patient never converted meaning the shock did not do its job at all. In this case, you should get a second defibrillator and perform double sequential external defibrillation (DSED). Simply attach a second defibrillator as shown in the diagram below and deliver max shocks from both devices simultaneously.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content