This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronaryarterydisease with supply/demand mismatch). The arterial blood gas showed a lactic acidosis with a lactate level of 17mmol/L. As per Dr.
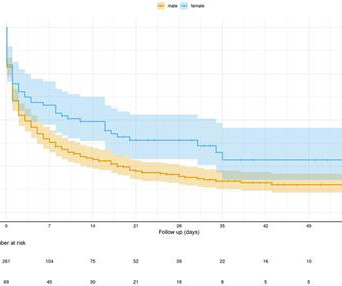
Female patients showed a lower prevalence rate of pre-existing coronaryarterydisease (48% vs. 75%, p < 0.001) and cardiomyopathy (17% vs. 34%, p = 0.01) compared with the male patients, while the mean age and prevalence rate of other cardiovascular risk factors were balanced.
Introduction The use of contemporary drug-eluting stents (DES) has significantly improved outcomes of patients with coronaryarterydisease (CAD) undergoing percutaneous coronary intervention (PCI). years, Diabetes mellitus 29%, acute coronary syndrome 67%, chronic total occlusion 9%).
We aimed to investigate the prevalence and outcomes of patients with SMuRF-less ACS undergoing percutaneous coronary intervention (PCI) compared with those with SMuRFs. Patients with coronaryarterydisease were excluded. vs 50.8%, p<0.001) and were more likely to experience postprocedural cardiogenicshock (4.5%
INTRODUCTION:Percutaneous coronary intervention for complex coronarydisease is associated with a high risk of cardiogenicshock. Cardiogenicshock and acute ST-segment–elevation myocardial infarction are exclusions. Circulation: Cardiovascular Interventions, Ahead of Print.
The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. Studies of patients with coronaryarterydisease who developed arrhythmic storm with episodes of PMVT following MI — show arrhythmias indistinguishable from those reported in this case.
The diagnostic coronary angiogram identified only minimal coronaryarterydisease, but there was a severely calcified, ‘immobile’ aortic valve. Authors' commentary: Cardiogenicshock in the setting of severe aortic stenosis. Fundamentally, cardiogenicshock is an issue of decreased cardiac output.
Clinical presentation was stable angina 130/567 (22.9%), non-ST-elevation acute coronary syndrome (NSTEACS) 312/567 (55%), ST-elevation myocardial infarction (STEMI) 125/567 (22.0%), and STEMI with cardiogenicshock 13/125 (10.4%). The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronaryarterydisease? Incidence of an acute coronary occlusion. 3-vessel disease? An elderly man with sudden cardiogenicshock, diffuse ST depressions, and STE in aVR Literature 1.
TIMI flow 0) is rare in the ED, as most either die before arrival or are recognized clinically due to cardiogenicshock. 61,66) In a patient with otherwise diagnostic STE, additional STE in aVR does not represent LM OMI and is not helpful in diagnosing the infarct-related artery or the site of occlusion.(67)
It’s essential for those at risk of coronaryarterydisease to be aware of the following symptoms. High cholesterol levels can clog your arteries, increasing the risk of coronaryarterydisease and heart attack. However, if the signs are not clear or severe, the patient may not respond quickly.
Whenever there is tachycardia, I am skeptical of OMI unless it has led to severely compromised ejection fracction with cardiogenicshock. The scan showed a bicuspid aortic valve with severe stenosis and coronaryarterydisease. Or I suspect that there is OMI simultaneous with another pathology.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content