This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. Author continued : STE in aVR is often due to left main coronaryartery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-ArterialCoronary Surgery: Ten Year Follow-up of One Million (..)
Program Designations Access and Publications (A&P) 1 Participant User File (PUF) 2 Task Force on Funded Research (TFR) 3 Special Projects 4 Adult Cardiac Surgery Database Lead Author Title Publication Date William Keeling 2 National Trends in Emergency CoronaryArteryBypassGrafting European Journal of Cardiothoracic Surgery October 2023 Jake (..)
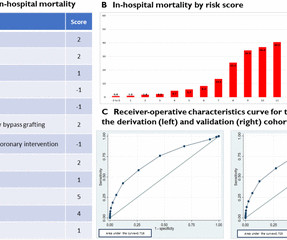
A novel risk score was developed, including the following parameters: male sex, age >70 years, non-white race, hypertension, hyperlipidemia, history of coronaryarterybypassgrafting, history of percutaneous coronary intervention, cardiac arrhythmias, renal failure, cardiogenicshock and vasopressor use.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chest pain and shortness of breath. Whenever there is tachycardia, I am skeptical of OMI unless it has led to severely compromised ejection fracction with cardiogenicshock. This was written by Hans Helseth.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content