This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Pendell Meyers A man in his 40s called EMS for acute chestpain that awoke him from sleep, along with nausea and shortness of breath. Long term outcome is unavailable. His history included known heart failure with prior EF 18%, insulin dependent diabetes, and polysubstance abuse.
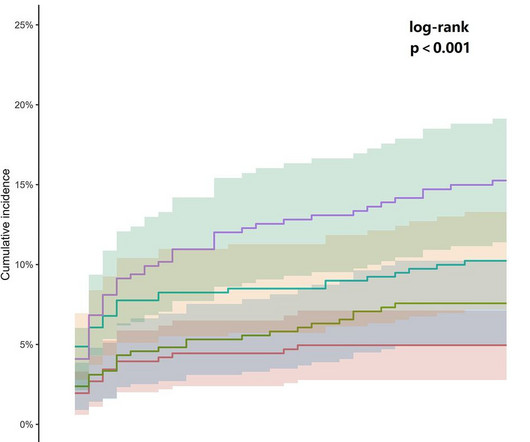
ObjectiveAlthough the association between admission glucose (AG) and major adverse cardiac events (MACE) is well-documented, its relationship with 30-day MACE in patients presenting with cardiac chestpain remains unclarified. The average age of the patients was 65.23 ± 12.66 years, The median AG levels were 7.60 mmol/L
Bad chest pressure with severe left shoulder pain 3 nights ago. Now appears to be in cardiogenicshock." However, cardiogenicshock usually takes some time to develop, so it is probably subacute." Cardiogenicshock and ACS is an indication for the cath lab, even if you don't think there is OMI.
A 50-something man presented in shock with severe chestpain. The patient was in clinical shock with a lactate of 8. His prehospital ECG was diagnostic of inferior posterior OMI. BP was 108 systolic (if a cuff pressure can be trusted) but appeared to be maintaining BP only by very high systemic vascular resistance.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." Lobo et al. examined SCAD presenting as STEMI (unlike Hassan et al.
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He was in cardiogenicshock requiring an impella for several days after cath.
This paper reports a case of an elderly female patient who experienced severe chestpain and syncope during acupuncture therapy, subsequently diagnosed with traumatic hemopericardium and acute cardiac tamponade, complicated by cardiogenicshock.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Queen of Hearts Interpretation: Would 20 minutes earlier diagnosis have made a difference in his clinical outcome?
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
This year’s theme, “Advancing Cardiovascular Care for All” brings the latest practice-changing breakthroughs, along with top experts debating and discussing outcomes of highly-anticipated clinical trials. 24 from April 6 - 8, 2024 in Atlanta, GA at the Georgia World Congress Center.
Just the fact of chestpain and highly elevated troponin is enough to activate the cath lab, but here you can see just how subtle hyperacute T-waves can be. 2) Typical persistent chestpain with a sigificantly elevated troponin is OMI until proven otherwise, regardless of the ECG.
All of the patients presented with chestpain , and they are all in triage. ECG#1 ECG#2 ECG#3 ECG#4 ECG#5 See outcomes of all 5 below, with the Queen of Hearts AI Bot interpretation. The patient died of cardiogenicshock within 24 hours despite mechanical circulatory support. YOU TOO CAN HAVE THE PM Cardio AI BOT!!
Then the notes mention "cardiogenicshock" but without any reference to a cardiac echo or to a chest x-ray. Now chestpain free. Cardiologist note says: "Elevated troponin explained by type II MI due to her shock." After midnight (now day 3), she complains of shoulder pain and dyspnea.
This is one case where it made a difference: Right Ventricular MI seen on ECG helps Angiographer to find Culprit Lesion Nevertheless, it is sometimes a fun academic exercise to try to predict the infarct artery: An elderly patient had onset of chestpain one hour prior. His included cardiogenicshock, V Tach, AV block.
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. such Q-waves are associated with larger MI and worse outcomes (2. There was some SOB. He had walked into the ED (did not use EMS). Obviously there is MI.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. An elderly man with sudden cardiogenicshock, diffuse ST depressions, and STE in aVR Literature 1.
His comments/questions are inserted below the ECG: A 50-something woman presented with 3 days of intermittent chestpain that became worse on the day of presentation, with diaphoresis and radiation to the left arm, as well as abdominal pain. This is her ECG: An obvious STEMI, but which artery?
When a person experiences a heart attack or myocardial infarction, they may feel chestpain and other symptoms in different parts of their body. It is imperative to act swiftly when faced with such a medical emergency to ensure the best possible outcome. So, how do you recognize a heart attack?
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Written by Willy Frick A woman in her 60s with very severe hyperlipidemia (LDL >200 mg/dL) presented with acute onset chestpain. She described the pain as moderate in severity, and said it had come and gone several times over the next few hours before ultimately resolving. Her symptoms began while getting off the bus.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content