This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). PIRP is strongly associated with myocardial rupture. The VSR is what is causing the cardiogenicshock! Heart rate was in the 80s.
A 50-something man presented in shock with severe chestpain. The patient was in clinical shock with a lactate of 8. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E.
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. I have always said that tachycardia should argue against acute MI unless there is cardiogenicshock or 2 simultaneous pathologies.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." Lobo et al. examined SCAD presenting as STEMI (unlike Hassan et al.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
ET Main Tent (Hall B1) - A Double-blind, Randomized Placebo Procedure-controlled Trial of an Interatrial Shunt in Patients with HFrEF and HFpEF: Principal Results From the RELIEVE-HF Trial - Empagliflozin After Acute MyocardialInfarction: Results of the EMPACT-MI Trial - CSL112 (Apolipoprotein A-I) Infusions and Cardiovascular Outcomes in Patients (..)
This is obviously diagnostic of inferior and lateral Occlusion MyocardialInfarction. The location of the infarct is clear, but that does not necessarily tell you what artery it is. Electrocardiographic diagnosis of acute coronary Occlusion MyocardialInfarction in ventricular paced rhythm using the modified Sgarbossa criteria.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Authors' commentary: Cardiogenicshock in the setting of severe aortic stenosis. Fundamentally, cardiogenicshock is an issue of decreased cardiac output.
This was my response: If it is the right clinical situation, such as acute chest discomfort, it looks like proximal left anterior descending occlusion with right bundle branch block and left anterior fascicular block. Because of the tachcardia, I would expect her to be very poor left ventricular function and maybe Cardiogenicshock.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. An elderly man with sudden cardiogenicshock, diffuse ST depressions, and STE in aVR Literature 1.
ObjectiveAlthough the association between admission glucose (AG) and major adverse cardiac events (MACE) is well-documented, its relationship with 30-day MACE in patients presenting with cardiac chestpain remains unclarified.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Why is there this notion that myocardialinfarction cannot be diagnosed in the setting of ventricular paced rhythm?
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
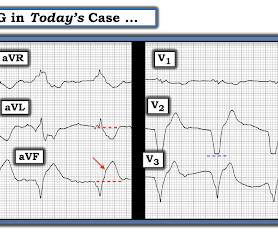
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. ng/ml and was falling, confirming infarction days ago. There was some SOB. He had walked into the ED (did not use EMS). Obviously there is MI. Hammill SC.
This pattern is essentially always accompanied by cardiogenicshock and high rates of VT/VF arrest, etc. The patient arrived to the ED in cardiogenicshock but awake. What is the Diagnosis in this 70-something with ChestPain? 68 minutes with chest compressions, full recovery. Eur Heart J.
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute MyocardialInfarction in the Emergency Department Case 1. Widimsky P et al. O'Gara PT, Kushner FG, Ascheim DD, et al.
When one of these arteries becomes completely blocked by a blood clot, it results in a heart attack, also known as MI (Myocardialinfarction). When a person experiences a heart attack or myocardialinfarction, they may feel chestpain and other symptoms in different parts of their body.
A middle-age woman with no previous cardiac history called 911 for chestpain. Primary VF in this study refers to fibrillation occurring in the absence of shock or pulmonary edema. This was her prehospital ECG: What do you think? The incidence varies from 2% to 19% depending on the definition of primary.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content