This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. His wife contacted the ambulance service after the patient experienced an episode of loss of consciousness.
Bad chest pressure with severe left shoulder pain 3 nights ago. Now appears to be in cardiogenicshock." This is ischemia until proven otherwise. However, cardiogenicshock usually takes some time to develop, so it is probably subacute." I was texted these ECGs. Then SOB and nausea the next day.
The VSR is what is causing the cardiogenicshock! Mechanical complications occur acutely and significantly alter hemodynamics leading to comp ensatory mechanism which usually involve vasoconstriction and tachycardia, both hallmarks of cardiogenicshock. PIRP is strongly associated with myocardial rupture.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." This strongly suggests reperfusing RCA ischemia. Lobo et al.
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). Here are some cases of RBBB with LAFB: What is the Diagnosis in this 70-something with ChestPain? There is STE in aVR.
The patient’s chestpain spontaneously resolved before he was evaluated and has a repeat ECG obtained at 22:12 obtained shown below. In context, of course, it is clear that the patient is reperfusing, as pain has dissipated and the diagnostic findings of OMI have become more nonspecific. This ECG is more difficult.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. For now she can only say Not OMI.
This 54 year old patient with a history of kidney transplant with poor transplant function had been vomiting all day when at 10 PM he developed severe substernal crushing chestpain. ACS and STEMI generally do not cause tachycardia unless there is cardiogenicshock. He had this ECG recorded. Are the lungs clear?
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. EKG shown here: LAFB with no clear signs of OMI or ischemia. Triage ECG: What do you think? This is a huge anterolateral OMI.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. There is no definite evidence of acute ischemia. (ie, The below ECG was recorded.
All of the patients presented with chestpain , and they are all in triage. Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. True Positive ECG#2 : Also sinus rhythm.
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chestpain and collapsed, and had bystander CPR. On arrival, GCS was 13 and the patient complained of ongoing chestpain. Vitals were HR 58 BP 167/70 R20 sat 96%.
A middle aged man had off and on chestpain for 2 weeks, then 2 hours of more severe and constant pain. Contrary to what Ken stated, the ST vector remains mostly posterior __ What about subendocardial ischemia? Similarly, STD in aVL is usually reciprocal to inferior ST elevation, not "lateral ischemia."
There is normal R-wave progression in the precordial leads with no evidence of ischemia. Just the fact of chestpain and highly elevated troponin is enough to activate the cath lab, but here you can see just how subtle hyperacute T-waves can be. Here the image quality is enhanced using the PM Cardio app. What do you think?
The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern). The patient arrived to the ED in cardiogenicshock but awake.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Anything more on history? J Electrocardiol 2013;46:240-8 2.
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. It should be known that each category can easily manifest the generic subendocardial ischemia pattern.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
This is one case where it made a difference: Right Ventricular MI seen on ECG helps Angiographer to find Culprit Lesion Nevertheless, it is sometimes a fun academic exercise to try to predict the infarct artery: An elderly patient had onset of chestpain one hour prior. His included cardiogenicshock, V Tach, AV block.
Then the notes mention "cardiogenicshock" but without any reference to a cardiac echo or to a chest x-ray. Now chestpain free. Cardiologist note says: "Elevated troponin explained by type II MI due to her shock." This is the etiology of the syncope and hypotension and shock and elevated CVP.
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
Written by Pendell Meyers An adult man presented with acute chestpain. The ECG shows sinus tachycardia, RBBB+LAFB, and signs of anterolateral acute transmural ischemia (most likely due to acute coronary occlusion), with concordant STE in I and aVL, inappropriate STE in V4-6 (though limited a bit by motion, still definite).
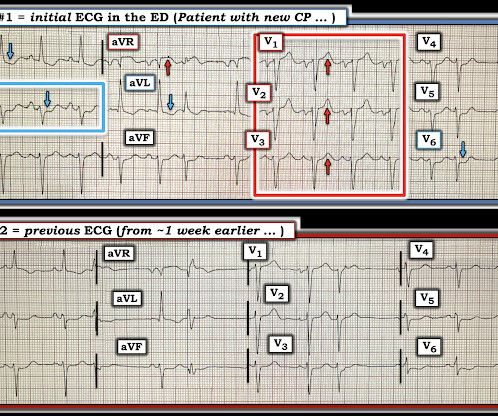
"Hi Steve wonder what you think of this ecg in a 60 yo woman w cp, known CAD" Presentation ECG (ECG 1): Here is her previous from one week prior when she presented with heart failure and trops were "negative" (ECG 2): My response: "They both look like active ischemia. The previous ECG also shows active ischemia." Just awful all around.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Written by Willy Frick A woman in her 60s with very severe hyperlipidemia (LDL >200 mg/dL) presented with acute onset chestpain. She described the pain as moderate in severity, and said it had come and gone several times over the next few hours before ultimately resolving. Her symptoms began while getting off the bus.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content