This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Past medical history included diabetes and hypertension.
The VSR is what is causing the cardiogenicshock! Mechanical complications occur acutely and significantly alter hemodynamics leading to comp ensatory mechanism which usually involve vasoconstriction and tachycardia, both hallmarks of cardiogenicshock. PIRP is strongly associated with myocardial rupture.
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He had history of prior MIs and CABG, as well as diabetes, hypertension, and hyperlipidemia.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. Left main? 3-vessel disease?
Written by Pendell Meyers A man in his 40s called EMS for acute chestpain that awoke him from sleep, along with nausea and shortness of breath. His history included known heart failure with prior EF 18%, insulin dependent diabetes, and polysubstance abuse. Vitals were within normal limits except for tachypnea.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. And then, 15 minutes later in today's case — this patient was in cardiogenicshock.
A patient in their 40s with type 1 diabetes mellitus and hyperlipidemia presented to the emergency department with 5 days of “flu-like” illness. They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They denied fever, cough, dyspnea, and sick contacts.
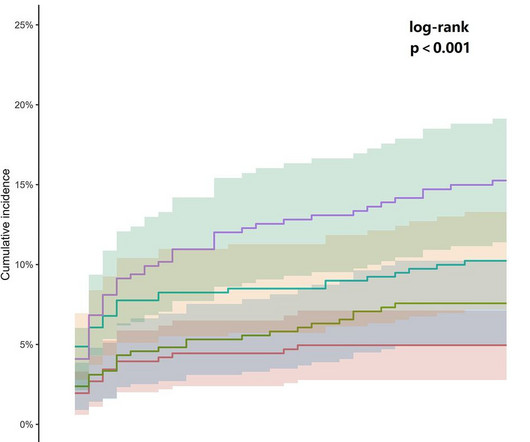
ObjectiveAlthough the association between admission glucose (AG) and major adverse cardiac events (MACE) is well-documented, its relationship with 30-day MACE in patients presenting with cardiac chestpain remains unclarified. years, with 1,028 (60.29%) being male and 500 (29.33%) having diabetes. The median AG levels were 7.60 mmol/L
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Sent by Pete McKenna M.D. Triage ECG: What do you think? This is diagnostic of proximal LAD occlusion. I cannot be anything else.
However, recent studies have observed that people below 40 are also experiencing heart attacks due to high blood pressure, cholesterol, diabetes, smoking, obesity, a sedentary lifestyle, and social and mental stress. Manage diabetes. Diabetes increases the risk of diabetic heart disease by a factor of two.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content