This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
High profile cases of sudden cardiacarrest in elite athletes in recent years has reminded the cardiology community of the challenging questions posed to cardiologists in these settings. Questions like: How do we prevent cardiacarrest in athletes? Can an athlete return to play after cardiacarrest?
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. The degree of stenosis is not a great predictor of thrombosis, and culprits may not be visible.
However, AKI patients had higher rates of deep vein thrombosis (6.36% vs. 3.54%, p < 0.01), pulmonary embolism (4.22% vs. 1.42%, p < 0.01), pneumonia (21.39% vs. 8.84%, p < 0.01), urinary tract infection (19.07% vs. 13.32%, p < 0.01), sepsis (20.27% vs. 4.18%, p < 0.01), acute myocardial infarction (12.14% vs. 3.21%, (..)
I suspect this is Type 2 MI due to prolonged severe hypotension from cardiacarrest. Coronary thrombosis or embolism can result in MINOCA, either with or without a hypercoagulable state. In non-arrest situations — escape beats and escape rhythms tend to be at least fairly regular.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. elevated BP), but rather directly correlated with coronary obstruction (due to plaque rupture and thrombosis) and, potentially, stymied TIMI flow. This results in Type I MI.
Thirty-six patients (36%) presented with cardiacarrest, and 78% (28/36) underwent emergent angiography. Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiacarrest; shock/profound hypotension; GI bleeding; anemia; "sick patient"; etc. ).
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow). He had multiple cardiacarrests with ROSC regained each time.
This case highlights such a scenario.Case:A 75-year-old female with a history of cardiacarrest 30 years ago presented with shortness of breath and left leg swelling. She experienced massive hemoptysis, leading to respiratory and cardiacarrest, but was resuscitated. Bronchoscopy revealed clots in the left lower lobe.
It was thought to be an in stent restenosis and thrombosis from a DES placed in the same region 6 months prior. Dialysis patients had double the rate of cardiacarrest (11% vs 5%), were less likely to receive reperfusion therapy when eligible (47% vs. 75%), and had an increased odds ratio of death compared to nondialysis patients 1.5 (95%
12,16 In 2017, CANTOS (Canakinumab Anti-inflammatory Thrombosis Outcomes Study) provided proof-of-principle that inflammation inhibition in the absence of lipid lowering can significantly reduce cardiovascular event rates and helped to define the interleukin-1 (IL-1) to IL-6 to CRP pathway as a central target in CV disease.16
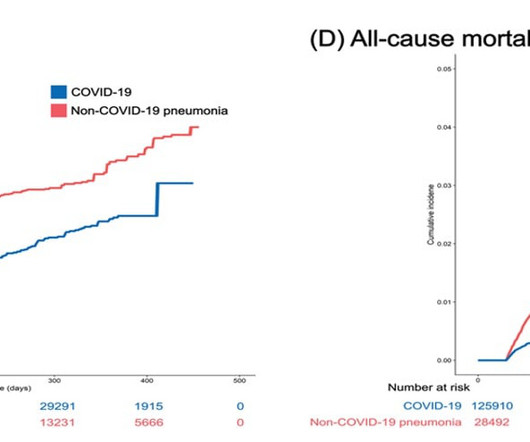
Imge courtesy of Won-Young Kim from Chung-Ang University milla1cf Thu, 01/11/2024 - 08:30 January 11, 2024 — Acute cardiovascular manifestations of COVID-19 , such as heart failure, thrombosis, and dysrhythmia, are associated with increased mortality.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content