This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia. Polymorphic ventricular tachycardia can be ischemic, catecholaminergic or related to QT prolongation. Cardiacarrest was called and advanced life support was undertaken for this patient. Without an MRI, it is impossible to know.
Then I always look to see if the initial deflection of the QRS has a lot of voltage change per change in time (seen in tachycardias that are initiated from above the ventricle because the propagate through fast conducting purkinje fiber. Tachycardia exaggerates ST Elevation in LBBB and Paced rhythm 5. Pacemaker mediated tachycardia!
Cingolani, director of Cardiogenetics and Preclinical Research in the Department of Cardiology in the Smidt Heart Institute at Cedars-Sinai, is exploring new ways to help patients with ventricular tachycardia (VT), a recurring, abnormally fast and irregular heartbeat that starts in the lower chambers, or ventricles, of the heart.
But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. See these related cases: Cardiacarrest, defibrillated, diffuse ST depression and ST Elevation in aVR.
There was concern that the rhythm might represent ventricular tachycardia, so lidocaine was given and one attempt at cardioversion was performed. A woman in her 50s with dyspnea and bradycardia A patient with cardiacarrest, ROSC, and right bundle branch block (RBBB). HyperKalemia with CardiacArrest.
While on telemetry monitoring he suffered cardiacarrest and was resuscitated. What ECG finding may have contributed to (or precipitated) the cardiacarrest? Learning points : Takotsubo can lead to cardiacarrest from ventricular arrhythmia. There are no clear signs of OMI. There is a prolonged QTc.
He developed cardiacarrest shortly after the ECG in Figure-1 was recorded. IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made. What is the most likely cause of this arrhythmia?
This is obviously severe hyperkalemia and the patient is near cardiacarrest. There was no IV access, so we obtained intraosseous (IO) access, but she arrested before we could give her all the calcium. Hyperkalemia and CardiacArrest Could you have prevented this young man's cardiacarrest?
Written by Pendell Meyers, with edits by Steve Smith Thanks to my attending Nic Thompson who superbly led this resuscitation We received a call that a middle aged male in cardiacarrest was 5 minutes out. There is a regular, wide complex, (mostly) monomorphic tachycardia. He was estimated to be in his 50s, with no known PMHx.
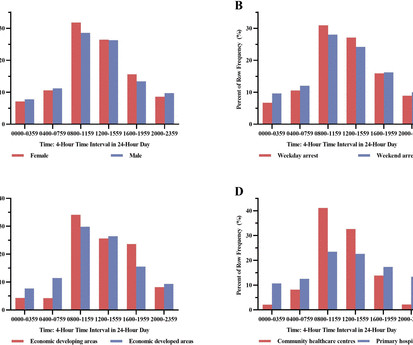
Background The circadian variation pattern of sudden cardiacarrest (SCA) occurred in Chinese community including both community healthcare centres and primary hospitals remains unknown. This study analysed the circadian variation of SCA in the Chinese community.
See this post: How a pause can cause cardiacarrest 2. Even with tachycardia and a paced QRS duration of ~0.16 There is ventricular bigeminy with bizarre appearing wide T-waves See even more striking cases of this at the bottom of the post. The plan: 1. Place temporary pacemaker 3. J Am Coll Cardiol.
We have recently reported that chronic kidney disease (CKD) is associated with higher likelihood of sudden cardiacarrest (SCA) presenting with non-shockable rhythms (NSR) (pulseless electrical activity/asystole), as opposed to shockable rhythms (ventricular fibrillation/pulseless ventricular tachycardia).
A 60-something woman presented after a witnessed cardiacarrest. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. Final Diagnosis: CardiacArrest due to Torsades from long QT of unknown etiology.
He had multiple cardiacarrests with ROSC regained each time. Then there is loss of pulses with continued narrow complex on the monitor ("PEA arrest") Learning Points: Sudden witnessed CardiacArrest due to ACS is almost always due to dysrhythmia. This patient arrested shortly after hospital arrival.
We received 4 ECGs, including his baseline on file, and three from today, including triage, peri-arrest, and post-ROSC (sorry for the poor quality due to scanning). Prior ECG on file: Sinus tachycardia, imperfect baseline, otherwise unremarkable. Unfortunately, this was not recognized at this time.
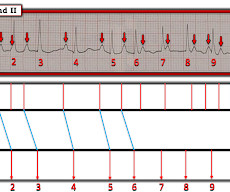
What is the cardiac rhythm shown in the long lead II rhythm strip? Figure-1: The initial ECG in today’s case — obtained from an elderly woman following successful resuscitation from cardiacarrest. ( C ASE C onclusion : I lack detailed follow-up from today's case — other than knowing that the Atrial Tachycardia was controlled.
This sinus tachycardia ( at ~130/minute ) — is consistent with the patient’s worsening clinical condition, with development of cardiogenic shock. Elevated troponin does not, however, guide any treatment strategies to minimize myocardial injury. The limb lead artifact ( from the “culprit” RA extremity ) had resolved.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. T wave alternans is a harbinger of cardiac instability and TdP. (3) No ischemic ST changes.
A small proportion of patients with STEMI treated via primary PCI experienced late ventricular tachycardia (VT) or ventricular fibrillation (VF), occurring one or more days following the procedure, but late VT or VF with cardiacarrest occurred rarely, especially among patients with uncomplicated STEMI, according to a study published in JAMA Network (..)
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Should you activate the cath lab?
Although one may have all kinds of ischemic findings as a result of cardiacarrest (rather than cause of cardiacarrest), this degree of ST elevation and HATW is all but diagnostic of acute proximal LAD occlusion. This prompted cath lab activation. On arrival to the ED, this ECG was recorded: What do you think?
BACKGROUND:In severely affected patients with catecholaminergic polymorphic ventricular tachycardia, beta-blockers are often insufficiently protective. The primary end point was AEs, defined as sudden cardiac death, sudden cardiacarrest, appropriate implantable cardioverter defibrillator shock, and arrhythmic syncope.
ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management CardiacArrest.
With increased genetic testing, sudden cardiacarrest (SCA) survivors who carry variants in the cardiac ryanodine receptor (RYR2) gene but do not have the pathognomonic findings of catecholaminergic polymorphic ventricular tachycardia (CPVT) on exercise testing were identified.
For long QT syndrome (LQTS) and catecholaminergic polymorphic ventricular tachycardia (CPVT), this stems both from prior guidelines that considered beta-blockers (a cornerstone of LQTS and CPVT treatment) to be a contraindication to allergen immunotherapy (AIT) and from hesitancy to use epinephrine during anaphylaxis, out of fear of triggering a LQTS- (..)
Cardiac sarcoidosis (CS), a rare condition characterized by non-caseating granulomas, can manifest with symptoms such as atrioventricular block and ventricular tachycardia (VT), as well as mimic inherited cardiomyopathies. A 48-year-old male presented with recurrent VT. Genetic testing identified a pathogenic mutation in PKP2.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. If a patient presents with chest pain and a normal heart rate, or with shockable cardiacarrest, then ischemic appearing ST elevation is STEMI until proven otherwise.
Blood was drawn , and the patient was promptly placed in a room to be seen — but on entering, the ED physician found her unresponsive in cardiacarrest. Do you see any indication on this ECG of WHY this patient was about to arrest? Is there any indication on this ECG of WHY this patient shortly after had a cardiacarrest?
The 2019 ESC Guidelines for the management of patients with supraventricular tachycardia indicated that IV Amiodarone should not be considered in these populations. Regarding AFib with WPW: The very rapid heart rate and at times extremely short R-R intervals put the patient with AFib and WPW at risk of cardiacarrest from VFib.
A few decades ago all sudden cardiacarrests with documented ventricular fibrillation (VF) and structurally normal hearts were diagnosed as idiopathic ventricular fibrillation (IVF).
This patient is actively dying from a left main coronary artery OMI and cardiacarrest from VT/VF or PEA is imminent! Complete LMCA occlusion is associated with clinical shock and/or cardiacarrest. The arterial blood gas showed a lactic acidosis with a lactate level of 17mmol/L.
See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades. If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 Could the dysrhythmias have been prevented? mEq/L, from 1.9
A man in his 30s with cardiacarrest and STE on the post-ROSC ECG == MY Comment , by K EN G RAUER, MD ( 12/31 /2023 ): == My only hope about today's tragic case — is that the involved providers learn from mistakes made. KEY Findings in ECG #1 include the following: Sinus tachycardia at ~110/minute. Junctional tachycardia? ).
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). The patient improved, and on Day-11 of the hospital stay — he was off inotropes and on a small dose of a ß-blocker. He required multiple defibrillations within a period of a few hours.
Here is the ECG: Sinus tachycardia. If cardiacarrest from hypokalemia is imminent (i.e., CASE : Prehospital CardiacArrest due to Hypokalemia I recently had a case of prehospital cardiacarrest that turned out to be due to hypokalemia. This patient presented with severe DKA. What do you think?
Examples of conditions notorious for producing arrhythmias that "do not obey the rules" include: i ) Hyperkalemia ( See ECG Blog #275 ) ; ii ) Cardiacarrest ; and , iii ) Vagotonic Block ( See ECG Blog #61 ).
A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. CardiacarrestCardiacarrest is a medical emergency in which the heart stops pumping blood to the body. Electrocardiogram, echocardiogram, and some other tests are done for patients with cardiacarrest.
Is it ventricular tachycardia (VT) due to hyperK or is it a supraventricular rhythm with hyperK? Here are other posts on hyperK, large calcium doses for hyperK, and ventricular tachycardia in hyperK Weakness, prolonged PR interval, wide complex, ventricular tachycardia Very Wide and Very Fast, What is it? How would you treat?
There is sinus tachycardia (do not be fooled into thinking this is VT or another wide complex tachycardia!) Plus recommendations from a 5-member panel on cardiacarrest. This feature is invaluable for assessing QRS morphology with wide tachycardias in the differentiation between SVT vs VT rhythms.
Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia. AI recognizing cardiacarrests in emergency calls. Recently, hospitals have failed to identify 25% of cases of cardiacarrest.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
Descriptive analysis of the ECG in today's case reveals a regular, narrow tachycardia at ~130/minute , without clear sign of sinus P waves. But the rate is ~130/minute — which is a bit fast for sinus tachycardia. So IF this is sinus tachycardia with a sinoventricular rhythm — then we have to explain WHY the rate is this fast.
There was 100% proximal LAD occlusion with TIMI 0 flow, and cardiacarrest in the cath lab. There is sinus tachycardia at ~100/minute. As often emphasized by Dr. Smith — sinus tachycardia is not a common finding with acute OMI unless something else is going on (ie, cardiogenic shock ). As per Dr.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content