
ECG Cases 48 – ECG Interpretation in Cardiac Arrest
ECG Cases
FEBRUARY 13, 2024
The post ECG Cases 48 – ECG Interpretation in Cardiac Arrest appeared first on Emergency Medicine Cases.

ECG Cases
FEBRUARY 13, 2024
The post ECG Cases 48 – ECG Interpretation in Cardiac Arrest appeared first on Emergency Medicine Cases.
Dr. Smith's ECG Blog
JULY 9, 2024
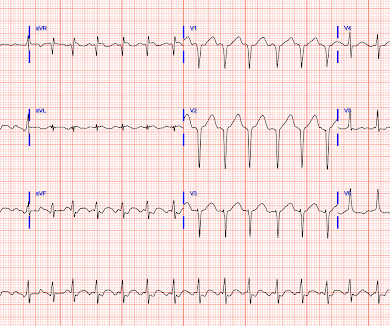
Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration. Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen.

Dr. Smith's ECG Blog
JULY 25, 2024
But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiac arrest, I ALWAYS wait 15 minutes after an ECG like this and record another. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR.

Dr. Smith's ECG Blog
SEPTEMBER 20, 2011
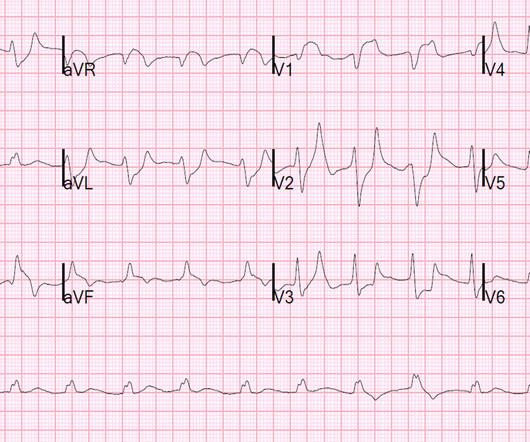
This 80 year old with a history of CABG had a cardiac arrest. This is as clear a STEMI as you can get. Now, it is true that shortly after a non-ACS cardiac arrest, there can be transient diffuse ST depression, but not ST elevation in a coronary distribution, and there should not be a wall motion abnormality.

American College of Cardiology
NOVEMBER 5, 2024
A small proportion of patients with STEMI treated via primary PCI experienced late ventricular tachycardia (VT) or ventricular fibrillation (VF), occurring one or more days following the procedure, but late VT or VF with cardiac arrest occurred rarely, especially among patients with uncomplicated STEMI, according to a study published in JAMA Network (..)

Dr. Smith's ECG Blog
APRIL 24, 2015
ST depression is common BOTH after resuscitation from cardiac arrest and during atrial fib with RVR. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. The patient was cardioverted. This was done.

Ken Grauer, MD
FEBRUARY 3, 2024
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiac arrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiac arrest. ( No CP ( C hest P ain ).

Expert insights. Personalized for you.






































Let's personalize your content