This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Photo by Cedars-Sinai milla1cf Fri, 03/01/2024 - 08:25 March 1, 2024 — Two new studies by Cedars-Sinai investigators support using artificial intelligence (AI) to predict sudden cardiacarrest-a health emergency that in 90% of cases leads to death within minutes.
The post EM Quick Hits 5 Ludwig’s Angina, Transient Monocular Vision Loss, D-dimer for PE Workup in Pregnancy, Pediatric Nasal Foreign Bodies, Trimethoprim Drug Interactions, Airway Management in CardiacArrest appeared first on Emergency Medicine Cases.
Despite the elevated mortality rates associated with high-risk pulmonary embolism (PE), this condition remains understudied. Data regarding the effectiveness and safety of invasive therapies such as venoarterial extracorporeal membrane oxygenation (VA-ECMO) in this patient population remains controversial.
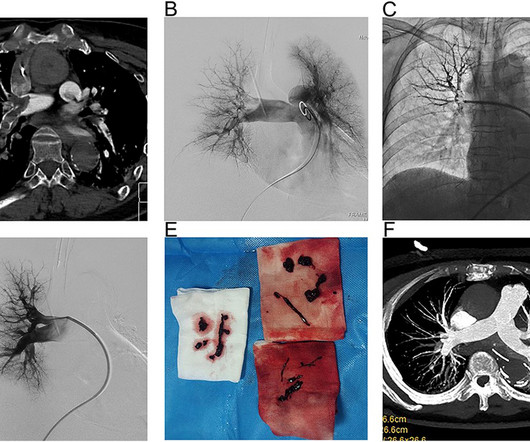
BackgroundPercutaneous mechanical thrombectomy (PMT) is increasingly used in the treatment of intermediate and high-risk acute pulmonary embolism (PE), and the treatment of high-risk PE with the aid of veno-arterial extracorporeal membrane oxygenation (VA-ECMO) has also been reported. The 12-month mortality rate was 36.4%.ConclusionVA-ECMO-assisted
High profile cases of sudden cardiacarrest in elite athletes in recent years has reminded the cardiology community of the challenging questions posed to cardiologists in these settings. Questions like: How do we prevent cardiacarrest in athletes? Can an athlete return to play after cardiacarrest?
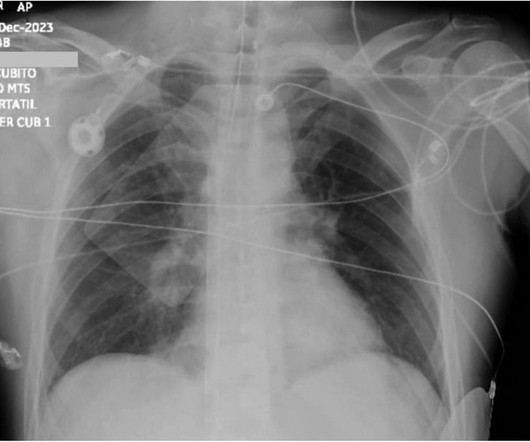
The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonary embolism). He had multiple cardiacarrests with ROSC regained each time. CT angiogram showed extensive saddle pulmonary embolism.
Background Data on the management of patients with cancer presenting with sudden cardiacarrest (SCA) are scarce. Cardiac causes were less frequent among patients with cancer (mostly acute coronary syndromes, 25.5% vs 46.8%, p<0.001) and had more respiratory causes (pulmonary embolism and hypoxaemia in 34.2%
I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiacarrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? Here is the troponin profile overnight: This is consistent with cardiacarrest without acute coronary occlusion. l/min cardiac output.
(MedPage Today) -- FDA alerted to Inari Medical's recall of instructions for use (IFU) of the ClotTriever XL catheter, 30 mm, following reports of injury and death due to entrapped devices or pulmonary emboli. A 3-month physical activity intervention.
Cardiogenic shock after outofhospital cardiacarrest (OHCA) can be due to transient myocardial stunning but also reflect the increasing severity of ongoing heart failure. The Society for Cardiovascular Angiography and Interventions (SCAI) proposed a division of cardiogenic shock into 5 phenotypes, with cardiacarrest being a modifier.
Massive pulmonary embolism (MPE) carries significant 30-day mortality and is characterized by acute right ventricular failure, hypotension, and hypoxia, leading to cardiovascular collapse and cardiacarrest.
Chronic Pulmonary Disease Lung diseases like chronic obstructive pulmonary disease (COPD) can lead to pulmonary hypertension, which in turn can cause the right side of the heart to enlarge, a condition known as cor pulmonale.
BackgroundAcute pulmonary embolism (APE) is a common and potentially fatal cardiovascular disease that can lead to sudden cardiacarrest in severe cases. For patients with concurrent main pulmonary artery embolism and bleeding, balloon pulmonary angioplasty may be an option.
The critical care management of patients after cardiacarrest is burdened by a lack of high-quality clinical studies and the resultant lack of high-certainty evidence. Critical care management is crucial in patients after cardiacarrest and affects outcome. Voting was anonymous and web based.
This false electrical capture may have made cardiacarrest recognition difficult, and the re-arrest may have gone unrecognized for an unknown amount of time. The receiving staff suspects pulmonary embolism due to S1Q3T3 on the ECG and administers TPA. On ED arrival ROSC is achieved.
and the patient was converted to veno-venous (V-V) ECMO due to persistent pulmonary insufficiency. Clinically — despite an initial 2-fold increased troponin, the normal bedside Echo was reassuring against OMI or pulmonary embolism. He remained supported on an intraaortic balloon pump. Here they are: Learning Points: 1.
The post EM Quick Hits 33 Polytrauma Tips & Tricks, Toxic Megacolon, ECG in PE, Patch Calls, CT Before LP, Nebulized Ketamine appeared first on Emergency Medicine Cases.
Although one may have all kinds of ischemic findings as a result of cardiacarrest (rather than cause of cardiacarrest), this degree of ST elevation and HATW is all but diagnostic of acute proximal LAD occlusion. This prompted cath lab activation. On arrival to the ED, this ECG was recorded: What do you think?
Patients with significant pulmonary oedema or aortic valve (AV) closure during venoarterial extracorporeal membrane oxygenation (VA-ECMO) were randomized to early left ventricular (LV) unloading or conventional strategy groups (1:1). The primary endpoint was the rate of weaning from VA-ECMO during index admission. vs. 1.7 ± 0.6
BACKGROUND:The aim of this study was to examine the impact of early versus delayed catheter-based therapies (CBTs) on clinical outcomes in patients with acute intermediate-risk pulmonary embolism (PE).METHODS:This Secondary outcomes included a composite of 30-day mortality, resuscitated cardiacarrest, and hemodynamic instability.
Introduction The use of venoarterial extracorporeal membrane oxygenation (VA-ECMO) in extracorporeal cardiopulmonary resuscitation (eCPR) has emerged as a treatment option for selected patients who are experiencing refractory cardiacarrest (CA).
Bedside cardiac ultrasound showed moderately decreased LV function. CT of the chest showed no pulmonary embolism but bibasilar infiltrates. See this post: How a pause can cause cardiacarrest 2. She was intubated. The plan: 1. Place temporary pacemaker 3. Discontinue amiodarone, since it prolongs the QT 4.
Blood was drawn , and the patient was promptly placed in a room to be seen — but on entering, the ED physician found her unresponsive in cardiacarrest. Do you see any indication on this ECG of WHY this patient was about to arrest? Is there any indication on this ECG of WHY this patient shortly after had a cardiacarrest?
Smith interpretation: This is highly likely to be due to extreme right heart strain and is nearly diagnostic of pulmonary embolism. What is the clear diagnosis and reason for arrest? It is of course pulmonary embolism. No d-dimer or CT pulmonary angiogram was done when they discovered that she had normal coronary arteries.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. Cardiac Motion Alternans — is the result of cardiac movement rather than electrical alternation.
I've previously discussed the interesting correlation of a qR pattern in lead V1 in patients with RVH — as strongly suggesting associated pulmonary hypertension ( See ECG Blog #234 and Blog #248 ). Unfortunately — the patient abruptly developed hypoxemia, followed by cardiacarrest with PEA. He could not be resuscitated.
This case highlights such a scenario.Case:A 75-year-old female with a history of cardiacarrest 30 years ago presented with shortness of breath and left leg swelling. She experienced massive hemoptysis, leading to respiratory and cardiacarrest, but was resuscitated. Bronchoscopy revealed clots in the left lower lobe.
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. I would do bedside ultrasound to look at the RV, look for B lines as a cause of hypoxia (which would support OMI, and argue against PE), and if any doubt persists, a rapid CT pulmonary angiogram.
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 He appeared to be in shock. mEq/L, from 1.9
The patient was slightly tachypneic and mildly hypoxic in the stabilization room and therefore the physicians obtained a CT pulmonary angiogram as well as aortogram to rule out dissection and PE. The initial Abbott hs troponin I returned at 52 ng/L (Upper reference limit for males is less than or equal to 34 ng/L). (Our
It makes pulmonary embolism (PE) very likely. The small LV implies very low LV filling pressures, which implies low pulmonary venous pressure. First, what kind of arrest was this? It was a PEA or bradyasystolic arrest , not a shockable rhythm. Possible, but huge pulmonary embolism is more likely. What is going on?
February 2024 FDA Approvals: Innovations in Cardiovascular Interventions XACT Carotid Stent System (Approved: 02/07/2024) This approval expands the indications to be used during a Transcarotid Artery Revascularization (TCAR) procedure to prevent future strokes.
Compared with 2012‐2014, the 2015‐2019 cohort showed increased odds of ICH and shock while the odds of DVT, pulmonary embolism, pneumonia, and UTI were significantly lower. Odds of a mild disability outcome increased from 16% to 20%, OR 0.65 (0.57, 0.74), while mortality decreased from 15% to 12%, OR 0.69 (0.61, 0.78).
However, AKI patients had higher rates of deep vein thrombosis (6.36% vs. 3.54%, p < 0.01), pulmonary embolism (4.22% vs. 1.42%, p < 0.01), pneumonia (21.39% vs. 8.84%, p < 0.01), urinary tract infection (19.07% vs. 13.32%, p < 0.01), sepsis (20.27% vs. 4.18%, p < 0.01), acute myocardial infarction (12.14% vs. 3.21%, (..)
CABANA Trial randomized 2204 patients with AF aged 65 years or more and those below 65 years with one or more risk factors for stroke for catheter ablation with pulmonary vein ablation or drug therapy with rate or rhythm control. Among the subjects of CABANA trial 35% had NYHA class above II at baseline. 2019 Apr 2;321(13):1261-1274.
I suspect this is Type 2 MI due to prolonged severe hypotension from cardiacarrest. pulmonary embolism, sepsis, etc.), PEARL: In my experience, cardiac rhythms observed during ( or shortly after ) cardiacarrest do not obey the usual rules for AV blocks and escape rhythms. myocarditis).
They include myocardial ischemia, acute pericarditis, pulmonary embolism, external compression due to mass over the right ventricular outflow tract region, and metabolic disorders like hyper or hypokalemia and hypercalcemia. These are the conditions which have to be considered or excluded as they can sometimes manifest Brugada pattern on ECG.
The estimated pulmonary artery systolic pressure is 29 mmHg + RA pressure. Conclusion: Type II MI probable due to hypoxia and tachycardia from resp arrest and amphetamine use. SUMMARY Normal left ventricular cavity size. Normal estimated left ventricular ejection fraction. No wall motion abnormality.
If a patient presents with chest pain and a normal heart rate, or with shockable cardiacarrest, then ischemic appearing ST elevation is STEMI until proven otherwise. The estimated pulmonary artery systolic pressure is 37 mmHg + RA pressure. Normal estimated left ventricular ejection fraction lower limits of normal.
Conduction and refractoriness alternans may be seen with WPW-related as well as AV Nodal-dependent reentr y tachycardias — atrial fibrillation — acute pulmonary embolus — myocardial contusion — and severe LV dysfunction. Cardiac Motion Alternans — is the result of cardiac movement rather than electrical alternation.
During the hospitalization, they had higher rates of renal failure, pulmonary artery catheter use, and mechanical circulatory support use. This was consistent across subgroups of CS cause, age, sex, hospital location, mechanical circulatory support use, and presence of cardiacarrest.
The patient was unconscious BEFORE the cardiacarrest, at the same time that she had strong pulses. Therefore, cardiacarrest is NOT the etiology of the coma. she had severe pulmonary edema. More cases here to highlight: [link] Middle Aged Woman with Asystolic CardiacArrest, Resuscitated: Cath Lab?
Chest X-ray also showed pulmonary edema. 1) as far as I can tell, there is very little data on amiodarone for this indication 2) amiodarone has beta blockade effects which could be deleterious in a patient with large anterior MI with pulmonary edema and at risk for cardiogenic shock (and she did go into shock. Potassium was 4.5
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content