This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background:In out-of-hospital cardiacarrest (OHCA) patients with an initial shockable rhythm, epinephrine increases the likelihood of return of spontaneous circulation (ROSC), but its effect on neurological outcome remains uncertain.
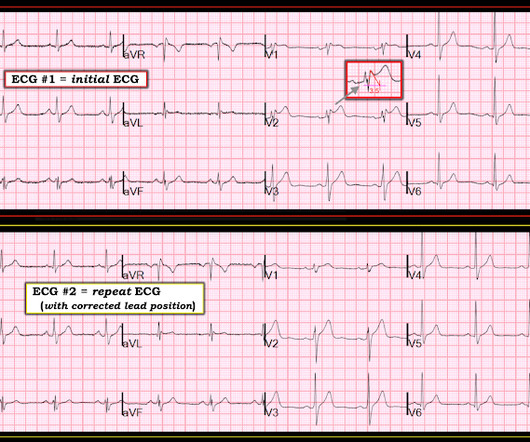
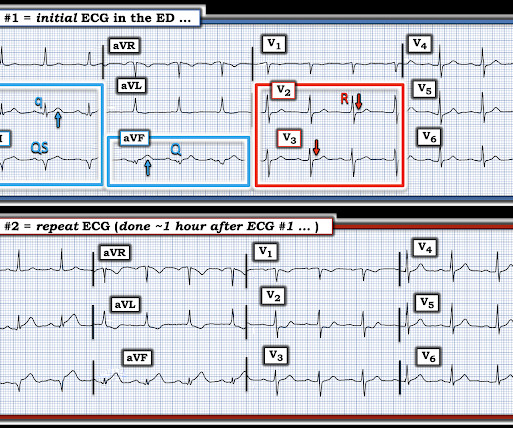
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. The described rhythm was an irregular, wide complex rhythm.
Hence, the IV Amiodarone was once one of the 2nd-line choices for acute pharmacologic cardioversion in such patients without hemodynamic instability. Regarding AFib with WPW: The very rapid heart rate and at times extremely short R-R intervals put the patient with AFib and WPW at risk of cardiacarrest from VFib.
If the rhythm converts and then reverts to tachycardia with either adenosine or electricity, Neither one of those modalities should be attempted until some longer acting pharmacological solution is given. WPW does not always have delta waves on the baseline ECG. This is called "Concealed conduction".
This may result from fluctuations in heart rate or in nervous system activity or from pharmacologic treatment. Conduction and Refractoriness Alternans — entails variance of impulse propagation along some par t of the conduction system.
If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 Crit Care Med 1991; 19:694) Concentrated Potassium Chloride Infusions in Critically Ill Patients with Hypokalemia The Journal of Clinical Pharmacology.
Intro:Mild hypothermia has proved clinically effective at improving outcomes in cardiacarrest patients for decades. Stroke, Volume 56, Issue Suppl_1 , Page ADP59-ADP59, February 1, 2025. Similarly, mild hypothermia has been shown to be neuroprotective in experimental stroke models. shiver response). shiver response).
Intro:Mild hypothermia has been clinically effective at improving outcomes in cardiacarrest patients for decades. To address a need for better strategies for cooling conscious subjects, we sought to promote mild hypothermia by pharmacological activation of heat-sensing nerve fibers in the thermoregulatory system.
When associated with appropriate clinical features (ie, personal history of cardiacarrest, polymorphic VT, non-vagal syncope, positive family history of sudden death at an early age, etc. ) — then spontaneous occurrence of a Brugada-1 ECG pattern is diagnostic of Brugada Syndrome.
mg experienced a 23% lower incidence of death from cardiovascular causes, resuscitated cardiacarrest, myocardial infarction, stroke, or urgent hospitalization for angina leading to coronary revascularization in a time-to-event analysis. Therapeutic potential of colchicine in cardiovascular medicine: a pharmacological review.
Pharmacological facilitation of primary percutaneous coronary intervention for acute myocardial infarction: is the slope of the curve the shape of the future? We are lucky this patient did not have a cardiacarrest while in the Waiting Room. JAMA [Internet] 2005;293(8):97986.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content