This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He had multiple cardiacarrests with ROSC regained each time. Dyspnea, Chest pain, Tachypneic, Ill appearing: Bedside Cardiac Echo gives the Diagnosis 31 Year Old Male with RUQ Pain and a History of Pericarditis. Cardiac Ultrasound may be a surprisingly easy way to help make the diagnosis Answer: pulmonary embolism.
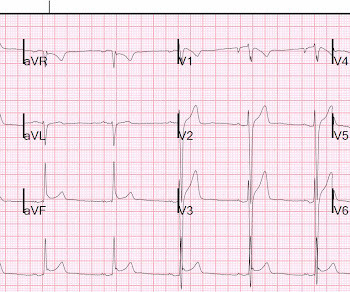
T-wave to ST ratio is greater than 4 in lead V6, making pericarditis unlikely (also there were no symptoms of pericarditis). If there are no changes in aVL, it is highly unlikely to be inferior STEMI. Would you be certain that it is not STEMI? Sudden cardiacarrest associated with early repolarization.
As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." Canto et al.
There is ST depression in II, III, and aVF that is concerning for reciprocal depression from high lateral STEMI in aVL, where there is some ST elevation. There is also ST depression in precordial leads, greatest in V3 and V4, concerning for posterior STEMI. The patient died is spite of resuscitative efforts. It is found on 1% to 3.5%
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chest pain, dyspnea and weakness on the treadmill. There is no acute STEMI. This is diagnostic of recent, reperfused STEMI. This is diagnostic of recent, reperfused STEMI. Acute STEMI would have upright T-waves.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content