This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiacarrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? Pacemaker mediated tachycardia! Another ECG was recorded 12 minutes later: Paced rhythm, probable Pacemaker-Mediated Tachycardia ?
Patients admitted on weekends also experienced higher rates of a range of complications: Paravalvular leakage (0.97% vs. 0.59%) Cardiogenic shock (7.59% vs. 3.97%) Permanent pacemaker implantation (11.12% vs. 9.25%) Endocarditis (0.74% vs. 0.37%) Cardiacarrest (2.19% vs. 1.65%) Acute kidney injury (29.76% vs. 19.56%) Acute ischemic stroke (2.94% vs. (..)
A 60-something woman presented after a witnessed cardiacarrest. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. Final Diagnosis: CardiacArrest due to Torsades from long QT of unknown etiology.
This is demonstrated ( Figure 5 ) by the gap in arrows at the bottom of the strip, signifying that the demand pacemaker has recognized an underlying rhythm (in this case, artifact from a moving ambulance). The artifact fools the pacemaker into thinking the rhythm is native. Current 85mA. They are unable to feel a pulse and resume CPR.
Patient had an unwitnessed cardiacarrest without bystander CPR performed. Figure 3 : TCP is started and the pacer spikes are followed by small phantom complexes and interspersed with native beats of the heart recognized by the demand pacemaker with a triangle and a pause in the pacer depolarization.
About 45 minutes after the second EKG, the patient was found in cardiacarrest. A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest.
Abstract Introduction The Medtronic Micra VR and Abbott AVEIR VR are the leadless pacemakers (LPM) currently available in the United States (US). The incidences of procedure-related death, cardiac perforation. cardiacarrest, emergency pericardial drainage or reparative surgery were similar for both LPMs ( p >.05).
See this post: How a pause can cause cardiacarrest 2. Place temporary pacemaker 3. The plan: 1. Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. Discontinue amiodarone, since it prolongs the QT 4.
An epicardial pacemaker was implanted. In 2012, she had a ventricular fibrillation cardiacarrest. In 1973 she underwent a Mustard operation, switching atrial blood flow using a baffle, which was complicated by complete heart block. The superior limb of the baffle was stenosed and required stenting.
Blood was drawn , and the patient was promptly placed in a room to be seen — but on entering, the ED physician found her unresponsive in cardiacarrest. Do you see any indication on this ECG of WHY this patient was about to arrest? Is there any indication on this ECG of WHY this patient shortly after had a cardiacarrest?
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. The described rhythm was an irregular, wide complex rhythm. Teaching Points: 1.
CardiacarrestCardiacarrest is a medical emergency in which the heart stops pumping blood to the body. Electrocardiogram, echocardiogram, and some other tests are done for patients with cardiacarrest. If the vital organs do not get their blood supply back quickly, it can lead to death.
My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. Given this patient's older age — if nothing "fixable" is found, she most likely has SSS ( S ick S inus S yndrome ) and will need a pacemaker ( See ECG Blog #342 for more on SSS ).
If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing"). Some residual ischemia in the infarct border might still be present. QUESTION: How will you handle this arrhythmia given the clinical scenario?
My thoughts were the following: ECGs #1 and #2 showed a completely unreliable sinus pacemaker, with presumed high-grade 2nd-degree AV block — and frequent resultant pauses of over 2 seconds ( that would have been even longer had it not been for intermittent relief from the atrial escape focus ). What Does this All Mean?
In fact, sometimes the sinus node is working and acting as a pacemaker but no P waves are visible!! These T-waves are tall but have a narrow base and a corresponding flat ST segment (see lead V4). Also, there are no definite P-waves and this is another result of hyperkalemia. This is called sino-ventricular rhythm. The patient was treated.
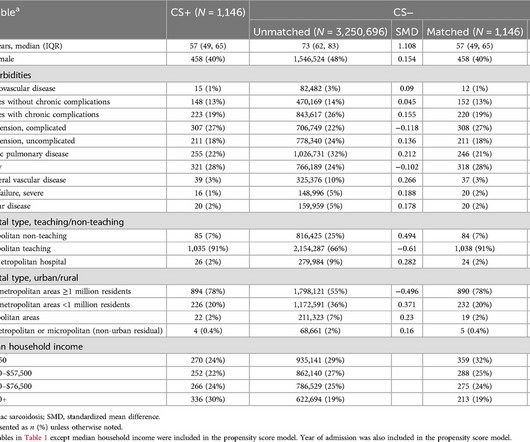
Hospitalizations with a primary diagnosis suggestive of CS (HF/cardiomyopathy, cardiacarrest, arrhythmias, or heart block) were categorized into cases with and without CS as a secondary diagnosis (CS+ and CS−, respectively).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content