This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Appreciation of these subtle ECG findings could have helped to avoid a cardiacarrest and its resulting permanent disability 3. Ischemia on the ECG can be very subtle and is easily missed. Accurate interpretation requires a lot of skill, practice, and experience.
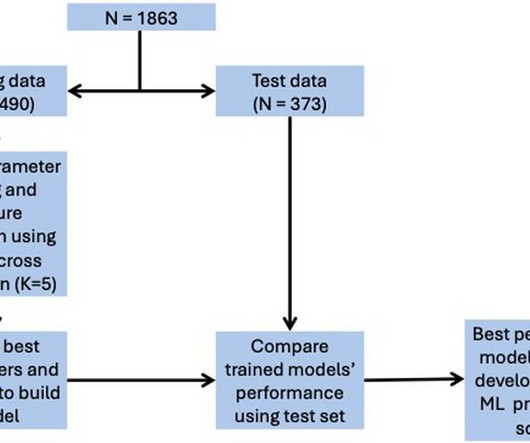
The included variables were age, pre-hospital cardiacarrest, robust collateral recruitment (Rentrop grade 2 or 3), family history of coronary disease, initial systolic blood pressure, initial heart rate, hypercholesterolemia, culprit vessel, smoking status and TIMI flow pre-PCI. for in-hospital mortality, 0.78 for LVEF < 40%.
Subtle as a STEMI." (i.e., About 45 minutes after the second EKG, the patient was found in cardiacarrest. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest. None of the 20 ever evolved to STEMI criteria.
Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. What is the utility of a head CT in cardiacarrest?
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardialinfarction (STEMI). We present the case of a man in his 50s, admitted with cardiacarrest secondary to inferolateral STEMI.
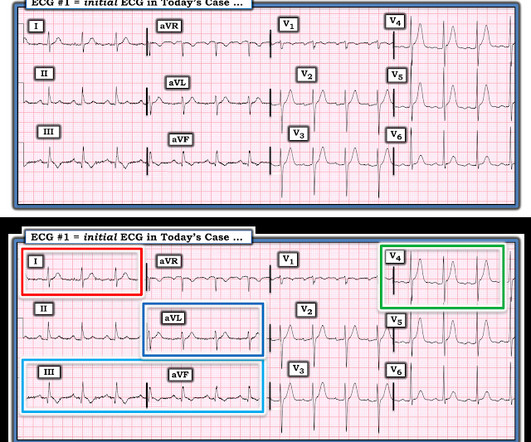
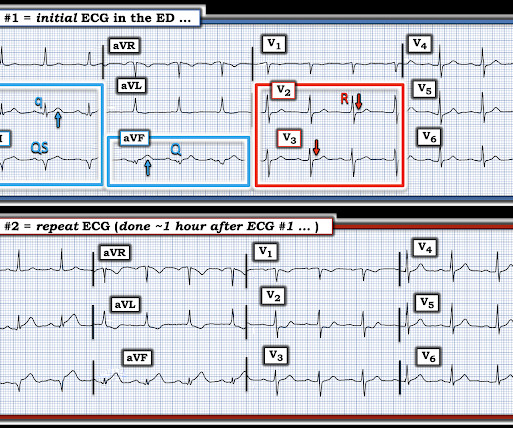
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
BackgroundThere may be variability in willingness to perform percutaneous coronary intervention (PCI) in higherrisk patients who present with STsegmentelevation myocardialinfarction (STEMI). There were 178 984 patients from 582 US hospitals presenting with STEMI who were included. versus 7.4%,P<0.001),
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. For this reason, some argue that it should not be measured in patients unless acute myocardialinfarction is on the differential diagnosis.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation.
BACKGROUND:Patients with ST-segment–elevation myocardialinfarction but no coronary microvascular injury are at low risk of early cardiovascular complications (ECC). CONCLUSIONS:NH-IMRangiois a valuable risk-stratification tool in patients with ST-segment–elevation myocardialinfarction.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Circulation 2007 2. Khan et al.
Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiacarrest with unrecognized STEMI, died. Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG.
The utility of the triage electrocardiogram for the detection of ST-segment elevation myocardialinfarction. link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise!
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). The below ECG was recorded. Inotropic medication was continued.
This is a troponin I level that is almost exclusively seen in STEMI. In this case, profound shock for 1 hour would result in the same degree of infarction. I suspect this is Type 2 MI due to prolonged severe hypotension from cardiacarrest. A followup ECG was recorded 2 days later: No definite evidence of infarction.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
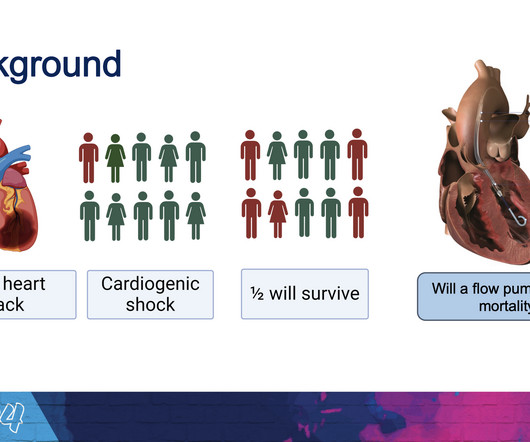
The new trial, called DanGer Shock , is the first trial powered to examine whether the use of micro-axial flow pumps can improve survival in ST-elevation myocardialinfarctions (STEMI, the most serious type of heart attack) that are complicated by cardiogenic shock.
If it is STEMI, it would have to be RBBB with STEMI. Only 5-18% of ED patients with chest pain have a myocardialinfarction of any kind. The patient presented with chest pain. Here is the ECG: What do you think? I frankly did not know what to think. Is it Brugada pattern? But in a very unusual pattern. Only 1-5% have OMI.
Technically, the STE meets STEMI criteria because there is greater than 2.5 These kinds of cases were excluded from the study as obvious anterior STEMI. Differences in electrocardiographic Findings Between Acute Isolated Right Ventricular MyocardialInfarction and Acute Anterior MyocardialInfarction.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries).
Both of these patterns together suggest Aslanger's pattern , recently published in J Electrocardiology: A new electrocardiographic pattern indicating inferior myocardialinfarction. Could this be Septal STEMI (STE in V1 and aVR, with reciprocal ST depression in V4-V6?), These suggest inferior OMI with possible RV involvement.
Acute myocardialinfarction in patients with dialysis Patients on dialysis have a well studied history of underdiagnosis and undertreatment for acute myocardialinfarction. Occlusion MyocardialInfarction (OMI) often does not present with diagnostic ST elevation, or even any STE, especially in dialysis patients.
This pattern is essentially always accompanied by cardiogenic shock and high rates of VT/VF arrest, etc. Code STEMI was activated. Plus recommendations from a 5-member panel on cardiacarrest. A man in his 80s with chest pain What, besides large anterior STEMI, is so ominous about this ECG? Eur Heart J.
There is worrisome T-wave inversion in inferior leads as well, which is another clue to LAD Occlusion In fact, this ECG meets STEMI criteria!! Why does the conventional algorithm not diagnose STEMI? Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chest pain, dyspnea and weakness on the treadmill. There is no acute STEMI. This is diagnostic of recent, reperfused STEMI. This is diagnostic of recent, reperfused STEMI. Acute STEMI would have upright T-waves.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
Here is the PMcardio Queen of Hearts interpretation of the ECG: STEMI equivalent detected. Inferior and posterior OMI without STEMI criteria. About an hour later another ECG was obtained: Barely meets STEMI criteria in inferior leads, but obvious inferior and posterior OMI. The cath lab was now activated for STEMI.
AimThis study aimed to protect brain functions in patients who experienced in-hospital cardiacarrest through the application of local cerebral hypothermia. underwent emergency coronary angiography due to ST-elevation myocardialinfarction (STEMI). Among the patients, 62.5%
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content