This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Curtain etal1 performed an analysis of the VALIANT (Valsartan in Acute MyocardialInfarction) and PARADISE-MI (Prospective ARNi vs ACE Inhibitor Trial to Determine Superiority in Reducing Heart Failure Events After MI) trials to evaluate whether risk of sudden cardiacarrest (SCA) following acute myocardialinfarction (MI) has changed over time.
Out-of-hospital cardiacarrest (OHCA) mostly occurs in crowded public places outside hospitals, such as public sports facilities, airports, railway stations, subway stations, and shopping malls. ECMO support therapy for patients with cardiacarrest can be considered when economic conditions permit.
BackgroundEarly coronary angiography (CAG) in post-cardiacarrest patients without ST-segment elevation is a topic of debate. A random-effects model pooled odds ratios (ORs) with 95% confidence intervals (CIs). Early CAG significantly reduced long-term mortality [OR: 0.66 (0.51–0.85)], Interpretation should be cautious.
Appreciation of these subtle ECG findings could have helped to avoid a cardiacarrest and its resulting permanent disability 3. Ischemia on the ECG can be very subtle and is easily missed. Accurate interpretation requires a lot of skill, practice, and experience.
Methods Predefined casecontrol sub-study within the international Targeted Hypothermia versus Targeted Normothermia after Out-of-Hospital CardiacArrest (TTM2) trial. OHCA survivors at 8 of 61 TTM2 sites in Sweden, Denmark and the United Kingdom were invited. Participants were matched 1:1 to MI controls.
Background Left ventricular free-wall rupture (LVFWR) is a catastrophic complication of acute myocardialinfarction (AMI). Historically, cardiac surgery is considered the treatment of choice. Low cardiac output syndrome was the main cause of postoperative death. The in-hospital mortality rate was 28.6%.
Background Out-of-hospital cardiacarrest (OHCA) has a dismal prognosis with overall survival around 10%. Previously, 80% of sudden cardiacarrest have been attributed to coronary artery disease. Survival curves were performed among hospitalised patients with acute myocardialinfarction (AMI) as well as heart failure.
The triglyceride-glucose (TyG) index, renowned for its efficacy and convenience in assessing insulin resistance, has been validated as a reliable indicator for various cardiovascular conditions. The current st.
What is the utility of a head CT in cardiacarrest? We found intracranial hemorrhage in 2% of non-traumatic cardiacarrest patients, and in 4 others the presence of cerebral edema changed management. in Vienna found that 27 of 765 (4%) of out of hospital cardiacarrests (OHCA) were due to SAH.
The study utilized the ISCHEMIA primary outcome, a composite measure of cardiovascular death, protocol-defined myocardialinfarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiacarrest. years, with 57.1% occurring within 30 days after CABG.
About 45 minutes after the second EKG, the patient was found in cardiacarrest. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest. Hyperacute T Wave in the Early Diagnosis of Acute MyocardialInfarction.
BackgroundCardiogenic shock complicating acute myocardialinfarction is associated with a high mortality rate. Cardiogenic shock after outofhospital cardiacarrest (OHCA) can be due to transient myocardial stunning but also reflect the increasing severity of ongoing heart failure.
Impella and venoarterial extracorporeal membrane oxygenation (VA-ECMO) in patients with acute myocardialinfarction-related cardiogenic shock (AMICS). Impella patients were older (34% vs. 13% >75 years, p < 0.001) and less frequently presented after an out-of-hospital cardiacarrest (18% vs. 40%, p < 0.001).
BACKGROUND:In patients with ST-segment–elevation myocardialinfarction complicated by cardiogenic shock, primary percutaneous coronary intervention (pPCI) is the preferred revascularization option. Circulation: Cardiovascular Interventions, Ahead of Print. pharmacoinvasive and 46.2% pharmacoinvasive and 46.2% pharmacoinvasive and 46.2%
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. For this reason, some argue that it should not be measured in patients unless acute myocardialinfarction is on the differential diagnosis.
BackgroundThere may be variability in willingness to perform percutaneous coronary intervention (PCI) in higherrisk patients who present with STsegmentelevation myocardialinfarction (STEMI). P<0.001), and more likely to have cardiacarrest before arrival (9.7% versus 7.4%,P<0.001), versus 5.1%,P<0.001)
BackgroundAcute myocardialinfarction complicated by cardiogenic shock (AMI‐CS) is associated with significant morbidity and mortality. mmol/L and cardiac power output was 0.67±0.29 watts. Journal of the American Heart Association, Volume 12, Issue 23 , December 5, 2023.
The cause of CS was acute myocardialinfarction in 438 (63.9%) patients, and 431 (62.9%) patients presented with cardiacarrest. interquartile range 4.112.7] A total of 410 patients (59.9%) were successfully weaned from VA-ECMO, whereas in 275 patients (40.1%) weaning failed (i.e.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation.
SMuRF-less patients were more likely to present with cardiacarrest (6.6% vs 3.9%, p<0.001) and ST-elevation myocardialinfarction (59.1% At 30 days, mortality, myocardialinfarction, revascularisation and major adverse cardiac and cerebrovascular events did not differ between the groups.
And pretty much every doctor can recall an event where a patient experienced a suddenly stressful event and had a cardiac event. That event might have been a heart rhythm issue or even a cardiacarrest. In the hours after the 911 attacks on the World Trade Centre in New York, the rates of cardiacarrest more than doubled.
If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 Literature on Hypokalemia as a risk for ventricular fibrillation in acute myocardialinfarction. mEq/L, and 10 mEq would increase it by 3.3 mEq/L, from 1.9
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardialinfarction (STEMI). We present the case of a man in his 50s, admitted with cardiacarrest secondary to inferolateral STEMI.
Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiacarrest with unrecognized STEMI, died. Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG.
The included variables were age, pre-hospital cardiacarrest, robust collateral recruitment (Rentrop grade 2 or 3), family history of coronary disease, initial systolic blood pressure, initial heart rate, hypercholesterolemia, culprit vessel, smoking status and TIMI flow pre-PCI. for in-hospital mortality, 0.78 for LVEF < 40%.
BACKGROUND:Patients with ST-segment–elevation myocardialinfarction but no coronary microvascular injury are at low risk of early cardiovascular complications (ECC). CONCLUSIONS:NH-IMRangiois a valuable risk-stratification tool in patients with ST-segment–elevation myocardialinfarction.
We evaluated the association between social vulnerability and a composite of myocardialinfarction, stroke, heart failure, venous thromboembolism, cardiogenic shock, cardiacarrest, and death, following discharge, using Cox regression models.
TTE showed a reduced EF with multiple segmental abnormalities concerning for myocardialinfarction. He had a cardiacarrest during the procedure and was placed back on ECMO. A repeat coronary angiogram was unremarkable. Intra-operative TEE showed an EF of 20% with no improvement after drainage.
They had had twice the rate of cardiacarrest and twice the in-hospital mortality[1] In another study of patients diagnosed with STEMI, those on dialysis experienced delayed reperfusion and double the mortality.[2] Clinical characteristics of dialysis patients with acute myocardialinfarction in the United States.
In this case, profound shock for 1 hour would result in the same degree of infarction. I suspect this is Type 2 MI due to prolonged severe hypotension from cardiacarrest. A followup ECG was recorded 2 days later: No definite evidence of infarction. This is a troponin I level that is almost exclusively seen in STEMI.
Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). Over the next couple of days the patient was weaned off of mechanical circulatory support. Inotropic medication was continued.
3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardialinfarction (MI), stroke, and cardiovascular (CV) death.4 Efficacy and Safety of Low-Dose Colchicine after MyocardialInfarction. 4 In the U.S. 12 Importantly, colchicine, 0.5 N Engl J Med.
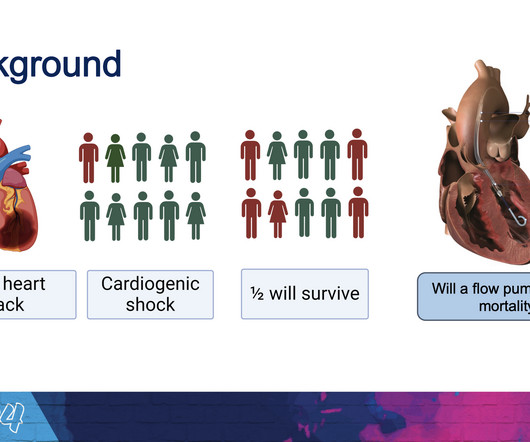
The new trial, called DanGer Shock , is the first trial powered to examine whether the use of micro-axial flow pumps can improve survival in ST-elevation myocardialinfarctions (STEMI, the most serious type of heart attack) that are complicated by cardiogenic shock.
However, AKI patients had higher rates of deep vein thrombosis (6.36% vs. 3.54%, p < 0.01), pulmonary embolism (4.22% vs. 1.42%, p < 0.01), pneumonia (21.39% vs. 8.84%, p < 0.01), urinary tract infection (19.07% vs. 13.32%, p < 0.01), sepsis (20.27% vs. 4.18%, p < 0.01), acute myocardialinfarction (12.14% vs. 3.21%, (..)
Acute myocardialinfarction in patients with dialysis Patients on dialysis have a well studied history of underdiagnosis and undertreatment for acute myocardialinfarction. Occlusion MyocardialInfarction (OMI) often does not present with diagnostic ST elevation, or even any STE, especially in dialysis patients.
The utility of the triage electrocardiogram for the detection of ST-segment elevation myocardialinfarction. Given the dire consequences of missing a STEMI or OMI, including cardiacarrest (see cases below), $5700 is extremely cheap. This paper was just published: Noll S. Am J Emerg Med 36(10):1771-1774. October 2018.
Differences in electrocardiographic Findings Between Acute Isolated Right Ventricular MyocardialInfarction and Acute Anterior MyocardialInfarction. As he was alarmed by it, he went to the patient who now was having recurrent pain, then suddenly went into cardiacarrest (ventricular fibrillation).
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries).
Only 5-18% of ED patients with chest pain have a myocardialinfarction of any kind. Could this be a coincidence that the patient was experiencing chest pain and upon ECG capture the atypical brugada pattern was found? Answer : History is insensitive and nonspecific. It helps a little bit. Only 1-5% have OMI. How can this be 'Not MI' ?
New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Here is the abstract: Background Identification of ST elevation myocardialinfarction (STEMI) is critical because early reperfusion can save myocardium and increase survival.
Other cases of LAD OMI with RBBB/LAFB: A man in his 40s who really needs you to understand his ECG CardiacArrest at the airport, with an easy but important ECG for everyone to recognize A woman in her 60s with 6 hours of chest pain, dyspnea, tachycardia, and hypoxemia Ventricular Fibrillation, ROSC after perfusion restored by ECMO, then ECG.
Both of these patterns together suggest Aslanger's pattern , recently published in J Electrocardiology: A new electrocardiographic pattern indicating inferior myocardialinfarction. These suggest inferior OMI with possible RV involvement.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content