This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ECG shows severe ischemia, possibly posterior OMI. But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another.
ST depression is common BOTH after resuscitation from cardiacarrest and during atrial fib with RVR. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiacarrest, after defibrillation, and after cardioversion. The patient was cardioverted. This was done.
This ECG is diagnostic of diffuse subendocardial ischemia. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. What is the utility of a head CT in cardiacarrest? Kurkciyan et al.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. This rules out subendocardial ischemia and is diagnostic of posterior OMI. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later?
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. Alternatively, it is a variant of diffuse subendocardial ischemia, with STE in V1 reciprocal to ST depression in inferior and lateral leads.
Such T-waves are almost always reciprocal to ischemia in the region of aVL (although aVL looks n ormal here) , and in a patient with chest pain are nearly diagnostic of ischemia. Ischemia on the ECG can be very subtle and is easily missed. Ischemia on the ECG can be very subtle and is easily missed. Lesson : 1.
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
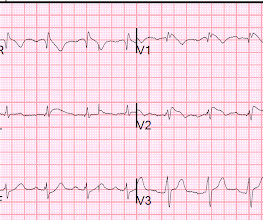
There is profound LVH with anterolateral ST elevation and reciprocal ST depression in II, III, aVF, and ST depression in V5 and V6 that could all be secondary to LVH or could represent ischemia superimposed on the repolarization abnormalities of LVH: note that wherever there is ST depression, it is associated with a very high voltage R-wave.
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. He had multiple cardiacarrests with ROSC regained each time.
911 was called and the medics recorded this ECG (unfortunately, leads V4-V6 are missing) Due to marked ST Elevation, the computer read was STEMI What do you think? See this post and associated case reports: Cardiacarrest, severe acidosis, and a bizarre ECG The patient was admitted and ruled out for acute MI by serial troponins.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management CardiacArrest.
In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 Available from: [link] 9. of Cardiology AC, Others. Troponin and BNP Use in COVID-19.
This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. If there is also subendocardial ischemia, the ST depression vector remains leftward, with a reciprocal ST Elevation vector also to the right.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. There is no definite evidence of acute ischemia. (ie, Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. ( The below ECG was recorded.
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiacarrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). To EMPHASIZE: This pattern of diffuse Subendocardial Ischemia does not suggest acute coronary occlusion ( ie, it is not the pattern of an acute MI ).
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
None of these findings are diagnostic of ischemia, but they should give you a high index of suspicion and prompt serial ECGs at a minimum. The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiacarrest. Anterolateral STEMI. Ischemia comes and goes.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
There is ST depression beyond the end of the wide QRS in I, II, aVF, and V4-V6, diagnostic of with subendocardial ischemia. It was a PEA or bradyasystolic arrest , not a shockable rhythm. LV anterior STEMI does not give maximal ST elevation in V1. So this ECG is typical of right ventricular (RV) STEMI. Summary: 1.
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. On arrival, GCS was 13 and the patient complained of ongoing chest pain.
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. This ECG was recorded prehospital, and the computer read STEMI, so the medics activated the cath lab: What do you think? The ECG is consistent with high lateral STEMI. Called 911.
This ST depression appears to be maximal in leads V3-to-V5 — which could reflect acute posterior OMI ( O cclusion-based M yocardial I nfarction ) — most probably with multi -vessel disease ( ie, diffuse subendocardial ischemia suggested by the ST depression with ST elevation in aVR>V1 ). This patient has new CP — and — he is hypotensive.
If it is STEMI, it would have to be RBBB with STEMI. Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada.
He has done a lot of great work on cardiacarrest, including as co-author of our study on esmolol in refractory cardiacarrest, and much more with Keith Lurie. The Queen was not able to see this one: Of course we do not know for certain that the inferior findings represent ischemia. It was not.
This ECG is all but diagnostic of subepicardial ischemia of the anterior, lateral, and inferior walls, most likely due to Occlusion MI (OMI), probably of the LAD. There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. Here is his ECG on arrival: What do you think?
He had a previous MI with cardiacarrest 2 years prior. Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. This is not normal and is a tip off that there is posterior ischemia accompanying the ischemia in aVL. Therefore it is not a STEMI.
The new trial, called DanGer Shock , is the first trial powered to examine whether the use of micro-axial flow pumps can improve survival in ST-elevation myocardial infarctions (STEMI, the most serious type of heart attack) that are complicated by cardiogenic shock. Overall, we have more complications, but we also save lives.”
Part of the ST depression with deep T wave inversion in the lateral chest leads clearly reflects LV "strain" from the marked LVH — but despite the very large QRS amplitudes, this ST-T wave appearance looks disproportionate, suggesting at least a component of ischemia. Then there is the significant ST elevation we see in lead V1.
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. A previous ECG from 4 years prior was normal: This looks like an anterior STEMI, but it is complicated by tachycardia (which can greatly elevate ST segments) and by the presentation which is of fever and sepsis.
The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern). Code STEMI was activated. This is "shark fin" morphology.
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". Hyperkalemia mimics STEMI and OMI in many distributions, but probably the most common is the Brugada morphology in V1-V2 which mimics anterior OMI for those who cannot recognize the Brugada pattern. HyperKalemia with CardiacArrest.
Normally, concavity in ST segments suggests absence of anterior ischemia (though concavity by itself is not reassuring - see this study ). In there ECG evidence of possible ongoing ischemia? (ie, IMPRESSION: I’d interpret this tracing as consistent with LVH and/or “strain” and/or ischemia. ie , Is it more than 50-60% likely? ).
A repeat ECG was done: Obvious anterolateral wall STEMI. This means that they occur shortly after onset of occlusion, but also may be the last remaining sign of ischemia after ST elevation resolves (after reperfusion). This rhythm reportedly produced no palpable pulse, and CPR was continued.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. BOTTOM Line: It can at times be extremely challenging to distinguish between anterior ST elevation from a benign Brugada Phenocopy pattern vs an acute anteroseptal STEMI.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Bicarb 20, Lactate 4.2,
There is ST depression in II, III, and aVF that is concerning for reciprocal depression from high lateral STEMI in aVL, where there is some ST elevation. There is also ST depression in precordial leads, greatest in V3 and V4, concerning for posterior STEMI. What was the inciting factor? The diagnosis is in doubt.
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chest pain, dyspnea and weakness on the treadmill. There is no acute STEMI. This is diagnostic of recent, reperfused STEMI. This is diagnostic of recent, reperfused STEMI. Acute STEMI would have upright T-waves.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! He was sent back to the waiting room, where he suffered a VF arrest. Approximately 5 minutes after ROSC, this ECG was obtained (about 45 minutes after arrival): Obvious anterolateral OMI, and STEMI criteria positive for those who care or need it.
A 12-lead was recorded, showing "STEMI," but is unavailable. The patient was unconscious BEFORE the cardiacarrest, at the same time that she had strong pulses. Therefore, cardiacarrest is NOT the etiology of the coma. She was BVM ventilated and suctioned. Shortly thereafter, pulses were lost.
The ECG shows sinus tachycardia, RBBB+LAFB, and signs of anterolateral acute transmural ischemia (most likely due to acute coronary occlusion), with concordant STE in I and aVL, inappropriate STE in V4-6 (though limited a bit by motion, still definite). Plus recommendations from a 5-member panel on cardiacarrest.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content