This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronary artery disease. years, with 57.1% occurring within 30 days after CABG. Original article: Redfors B et al.
Such T-waves are almost always reciprocal to ischemia in the region of aVL (although aVL looks n ormal here) , and in a patient with chest pain are nearly diagnostic of ischemia. Ischemia on the ECG can be very subtle and is easily missed. Ischemia on the ECG can be very subtle and is easily missed. Lesson : 1.
This ECG is diagnostic of diffuse subendocardial ischemia. What is the utility of a head CT in cardiacarrest? We found intracranial hemorrhage in 2% of non-traumatic cardiacarrest patients, and in 4 others the presence of cerebral edema changed management. We studied this and published the abstract below in 2010.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. For this reason, some argue that it should not be measured in patients unless acute myocardialinfarction is on the differential diagnosis.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation.
If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2
This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. If there is also subendocardial ischemia, the ST depression vector remains leftward, with a reciprocal ST Elevation vector also to the right.
Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). There is no definite evidence of acute ischemia. (ie, Some residual ischemia in the infarct border might still be present.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
They had had twice the rate of cardiacarrest and twice the in-hospital mortality[1] In another study of patients diagnosed with STEMI, those on dialysis experienced delayed reperfusion and double the mortality.[2] Clinical characteristics of dialysis patients with acute myocardialinfarction in the United States.
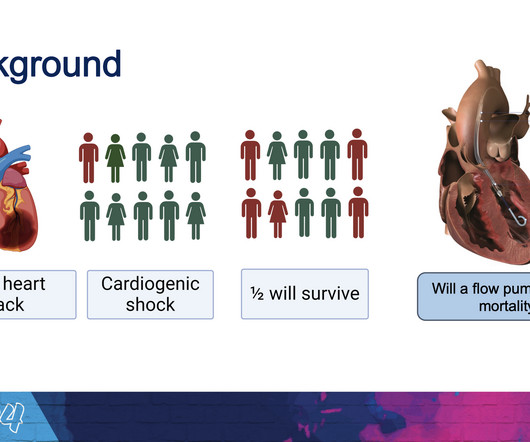
The new trial, called DanGer Shock , is the first trial powered to examine whether the use of micro-axial flow pumps can improve survival in ST-elevation myocardialinfarctions (STEMI, the most serious type of heart attack) that are complicated by cardiogenic shock. Overall, we have more complications, but we also save lives.”
Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada. Ischemia/infarction. It helps a little bit.
Normally, concavity in ST segments suggests absence of anterior ischemia (though concavity by itself is not reassuring - see this study ). Acute myocardialinfarction in patients with dialysis Patients on dialysis have a well studied history of underdiagnosis and undertreatment for acute myocardialinfarction.
3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardialinfarction (MI), stroke, and cardiovascular (CV) death.4 Efficacy and Safety of Low-Dose Colchicine after MyocardialInfarction. 4 In the U.S. 12 Colchicine, 0.5 34 Colchicine, 0.5 N Engl J Med.
The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern). Plus recommendations from a 5-member panel on cardiacarrest.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries).
The highly impactful International Study of Comparative Health Effectiveness With Medical and Invasive Approaches ( ISCHEMIA ) trial investigated the effectiveness of invasive (INV) versus conservative (CON) strategies for managing stable coronary artery disease. EuroIntervention. 2024 Mar 5:EIJ-D-24-00011.
We evaluated the primary outcome (cardiovascular death, myocardialinfarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiacarrest) and other end points, by sex, in 1168 (22.6%) women and 4011 (77.4%) men. of invasive‐assigned women revascularized versus 81.2%
The patient might be having cardiacischemia, but if he is, it is unstable angina or non-STEMI, or perhaps he has not YET pseudonormalized, so serial ECGs may be important. Differential of peri-infarct pericardial fluid The differential includes 1) pericarditis with effusion or 2) hemopericardium. These patients may survive.
Clinical questions : Is this an occlusion myocardialinfarction and does the patient need the cath lab? Occurrence of “J Waves” in 12-Lead ECG as a Marker of Acute Ischemia and Their Cellular Basis. Occurrence of "J waves" in 12-lead ECG as a marker of acute ischemia and their cellular basis. Pacing Clin Electrophysiol.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content