This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Cardiacarrest was called and advanced life support was undertaken for this patient. The patient was given chest compressions while waiting for the cardiacarrest team to arrive. Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. Calcium level was normal.
The ECG shows severe ischemia, possibly posterior OMI. But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another.
ST depression is common BOTH after resuscitation from cardiacarrest and during atrial fib with RVR. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiacarrest, after defibrillation, and after cardioversion. The patient was cardioverted. This was done.
Such T-waves are almost always reciprocal to ischemia in the region of aVL (although aVL looks n ormal here) , and in a patient with chest pain are nearly diagnostic of ischemia. Ischemia on the ECG can be very subtle and is easily missed. Ischemia on the ECG can be very subtle and is easily missed. Lesson : 1.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
A 60-something woman presented after a witnessed cardiacarrest. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. Final Diagnosis: CardiacArrest due to Torsades from long QT of unknown etiology.
Although one may have all kinds of ischemic findings as a result of cardiacarrest (rather than cause of cardiacarrest), this degree of ST elevation and HATW is all but diagnostic of acute proximal LAD occlusion. This rules out subendocardial ischemia and is diagnostic of posterior OMI. V4-5 continue to show STD.
There is profound LVH with anterolateral ST elevation and reciprocal ST depression in II, III, aVF, and ST depression in V5 and V6 that could all be secondary to LVH or could represent ischemia superimposed on the repolarization abnormalities of LVH: note that wherever there is ST depression, it is associated with a very high voltage R-wave.
The H ISTORY in T oday's C ASE: The patient in today's case is a teenager who presented to the ED ( E mergency D epartment ) in cardiacarrest after electrocution. Shark Fin" ST segment elevation is most often a sign of severe transmural ischemia that results from acute coronary occlusion.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation.
The ECG does not show any definite signs of ischemia. Uncontrolled coronary spasm may be associated with serious arrhythmias , including cardiacarrest ( Looi et al — Postgrad Med, 2012 ; Tan et al — Eur Heart J Case Rep, 2018 ; Chevalier et al — JACC, 1998 ; Rodriguez-Manero — EP Europace, 2018 ). The below ECG was recorded.
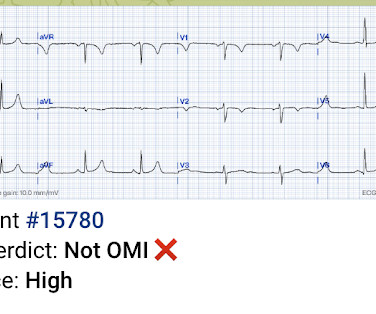
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
We periodically review this intriguing ECG finding that is best known for its association with hypothermia — but which may also be seen in association with a number of other entities, including acute infarction and cardiacarrest. My Comment addresses a few additional aspects of this phenomenon.
This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. If there is also subendocardial ischemia, the ST depression vector remains leftward, with a reciprocal ST Elevation vector also to the right.
Background:The incidence of cardiacarrest (CA) increases with age, leading to poorer neurological outcomes after the return of spontaneous circulation (ROSC) in the elderly.
See this post: How a pause can cause cardiacarrest 2. It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. The plan: 1. Place temporary pacemaker 3.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. The described rhythm was an irregular, wide complex rhythm.
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiacarrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). To EMPHASIZE: This pattern of diffuse Subendocardial Ischemia does not suggest acute coronary occlusion ( ie, it is not the pattern of an acute MI ).
None of these findings are diagnostic of ischemia, but they should give you a high index of suspicion and prompt serial ECGs at a minimum. The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiacarrest. Ischemia comes and goes. He was defibrillated. Anterolateral STEMI.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. So there is now high pre-test probability + refractory ischemia + Modified Sgarbossa + dynamic ECG changes. VF arrest is of course "electrical instability"! Learning points 1.
It should be known that each category can easily manifest the generic subendocardial ischemia pattern. In general, subendocardial ischemia is a consequence of global supply-demand mismatch that usually ameliorates upon addressing, and mitigating, the underlying cause. What’s interesting is that the ECG can only detect ischemia.
The differential is: Posterolateral OMI or subendocardial ischemia The distinction between posterior OMI and subendocardial ischemia can be important and sometimes difficult. Ischemic ST depression includes posterior OMI and subendocardial ischemia. Her prior ECG on file is shown below: What are your next steps?
He had a previous MI with cardiacarrest 2 years prior. Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. This is not normal and is a tip off that there is posterior ischemia accompanying the ischemia in aVL. This ECG is diagnostic of ischemia.
He has done a lot of great work on cardiacarrest, including as co-author of our study on esmolol in refractory cardiacarrest, and much more with Keith Lurie. The Queen was not able to see this one: Of course we do not know for certain that the inferior findings represent ischemia. It was not.
hours ECG: Not much change hs troponin I peaks at 500 ng/L 8 hours Next morning Urine drug screen: Amphetamine, Methamphetamine, Fentanyl, Fentanyl metabolite Formal Bubble Contrast Echocardiogram: Indications for Study: Silent Ischemia. Conclusion: Type II MI probable due to hypoxia and tachycardia from resp arrest and amphetamine use.
They had had twice the rate of cardiacarrest and twice the in-hospital mortality[1] In another study of patients diagnosed with STEMI, those on dialysis experienced delayed reperfusion and double the mortality.[2] They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
Common explanations for unusual rhythms such as this one include: i ) Hyperkalemia ( or other severe electrolyte disorder ); ii ) Recent infarction/ischemia; iii ) Sleep apnea; iv ) Severe hypothyroidism; v ) Acute neurologic catastrophe (ie, stroke, bleed, trauma, tumor ); vi ) Some other toxicity.
As discussed in ECG Blog #108 — AIVR generally occurs in one of the following C linical S ettings : i ) As a rhythm during cardiacarrest; ii ) In the monitoring phase of acute MI ( especially with inferior MI ) ; or , iii ) As a reperfusion arrhythmia ( ie, following thrombolysis, acute angioplasty, or spontaneous reperfusion ).
This means that they occur shortly after onset of occlusion, but also may be the last remaining sign of ischemia after ST elevation resolves (after reperfusion). Smith likes to say: "Hyperacute T-waves occur 'on the way up,' and 'on the way down.'"
This suggests ischemia of uncertain duration. Unfortunately, before this could be accomplished — the patient went into cardiacarrest. She was successfully resuscitated — with a post-arrest rhythm similar to that seen in Figure-1. Cardiac cath did not reveal significant coronary disease!
If a patient presents with chest pain and a normal heart rate, or with shockable cardiacarrest, then ischemic appearing ST elevation is STEMI until proven otherwise. It is prudent to treat the other conditions, get the heart rate controlled, and repeat the ECG.
This is often quite challenging to recognize — but the finding of negative U waves in a patient with chest pain is highly suggestive of ischemia ! N OTE # 2 — On rare occasions, the U wave may be negative. Figure-2: Sequential development of ST-T wave changes with hypokalemia. Note increasing U wave amplitude ( See text ).
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronary artery disease. years, with 57.1% occurring within 30 days after CABG. Original article: Redfors B et al.
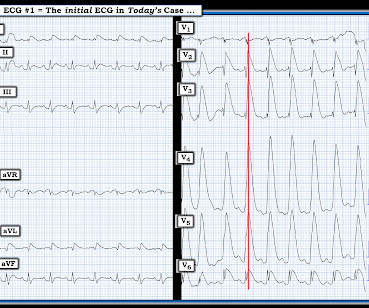
What is the cardiac rhythm shown in the long lead II rhythm strip? Figure-1: The initial ECG in today’s case — obtained from an elderly woman following successful resuscitation from cardiacarrest. ( To improve visualization — I've digitized the original ECG using PMcardio ). What about the 1 2- L ead E CG ?
Case submitted by Magnus Nossen MD from Norway, written by Pendell Meyers A man in his 50s with no pertinent medical history suffered a witnessed cardiacarrest. 12 minutes later, the patient went back into VFib arrest and underwent another 15 minutes of resuscitation followed by successful defibrillation and sustained ROSC.
Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. The above said — Electrical alternans is a nonspecific ECG sign that may also indicate myocardial ischemia, LV dysfunction and/or possibility of any of a number of other precipitating factors.
NOTE #3: In the context of a long QTc or ischemia — the finding of ST segment and/or T wave alternans may predict the occurrence of malignant ventricular arrhythmias.
These include ( among others ) — acute febrile illness — variations in autonomic tone — hypothermia — ischemia-infarction — malignant arrhythmias — cardiacarrest — and especially Hyperkalemia. Patients with such conditions that may transiently mimic the ECG findings of a Brugada-1 pattern are said to have Brugada Phenocopy.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. She was defibrillated and resuscitated. Smith: this ECG and clinical presentation is diagnostic of LAD Occlusion.
Use of objective evidence of myocardial ischemia to facilitate the diagnostic and prognostic distinction between type 2 myocardial infarction and myocardial injury. Any of these entities may result in myocardial “ stunning ” ( ie, transient marked reduction in cardiac contractility, that occurs in response to a major acute insult ).
He developed cardiacarrest shortly after the ECG in Figure-1 was recorded. Acute myocardial ischemia. Cardiac Sarcoidosis. Primary Cardiac Tumors and/or Cardiac Metastasis. C ASE C onclusion: As noted above — today's patient developed cardiacarrest shortly after arrival in the ED.
This ECG is diagnostic of diffuse subendocardial ischemia. What is the utility of a head CT in cardiacarrest? We found intracranial hemorrhage in 2% of non-traumatic cardiacarrest patients, and in 4 others the presence of cerebral edema changed management. We studied this and published the abstract below in 2010.
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. He had multiple cardiacarrests with ROSC regained each time.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content