This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
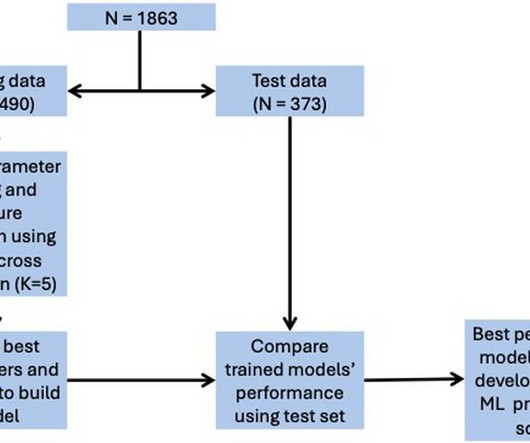
Final models were chosen to optimise area under the curve (AUC) score while ensuring interpretability.ResultsOverall, 128 (6.9%) patients died in hospital, with 292 (15.7%) patients requiring ICU admission and 373 (20.0%) patients with LVEF < 40%. for ICU admission, and 0.74 for in-hospital mortality, 0.78 for LVEF < 40%.
Subtle as a STEMI." (i.e., About 45 minutes after the second EKG, the patient was found in cardiacarrest. A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. Later the next day, she went into cardiacarrest again. None of the 20 ever evolved to STEMI criteria.
The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management CardiacArrest. Is it STEMI? What does the ECG show? Also see the bizarre Bigeminy.
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". He was admitted to the ICU and transferred emergently to a facility where he could undergo emergent dialysis as a part of further evaluation and management. Steve, what do you think of this ECG in this CardiacArrest Patient?"
Fortunately, he was extubated several days later in the ICU with intact baseline mental status and was discharged shortly thereafter to subacute rehab. His troponin I peaked at 97 ng/mL (very large MI!). His follow up ECHO the next day revealed an EF of 24% and a posterior wall motion abnormality.
and the patient was given more insulin/dextrose/calcium and admitted to ICU. 2] Curiously, ACLS does not include consideration of calcium in its bradycardia algorithm, which could have prevented the arrest and which along with the epi produced ROSC. HyperKalemia with CardiacArrest. References 1. Lindner et al.
The paramedics diagnosis was "Possible Anterolateral STEMI." More proof that a huge STEMI may have normal or near normal initial troponin. A retrospective 'target trial emulation' comparing amiodarone and lidocaine for adult out-of-hospital cardiacarrest resuscitation. The final angiographic result is very good.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content