This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Pendell Meyers, with edits by Steve Smith Thanks to my attending Nic Thompson who superbly led this resuscitation We received a call that a middle aged male in cardiacarrest was 5 minutes out. No other cause of arrest was identified based on lab results or pan-CT scan.
One hour later (labs not yet returned), here is the ECG recorded just after the team noticed a sudden wide complex with precipitous decompensation, just before cardiacarrest: Bizarre, Brady, and Broad (wide QRS). Upon arrival in the ICU, before getting Continuous Veno-Venous Hemodialysis (CVVHD), his potassium had risen again to 7.8
His temperature was brought back to normal over time in the ICU. C), with Cardiac Echo -- A Pathognomonic ECG. Norepinephrine was started, and another ECG was recorded: The patient was rewarmed with external rewarming, heated humidified air via ventilator circuit, warm IV fluid, and Arctic sun device. He did well and was discharged.
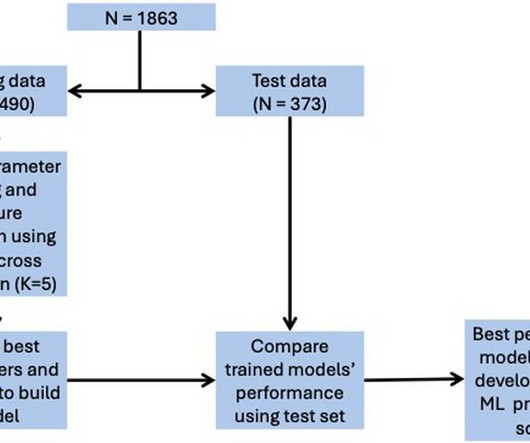
Final models were chosen to optimise area under the curve (AUC) score while ensuring interpretability.ResultsOverall, 128 (6.9%) patients died in hospital, with 292 (15.7%) patients requiring ICU admission and 373 (20.0%) patients with LVEF < 40%. for ICU admission, and 0.74 for in-hospital mortality, 0.78 for LVEF < 40%.
About 45 minutes after the second EKG, the patient was found in cardiacarrest. A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest.
CASE CONTINUED She was admitted to the ICU. See this post: How a pause can cause cardiacarrest 2. Smith has provided excellent overview of measuring and correcting QT interval in scenarios where QRS duration is prolonged (e.g., LBBB, ventricular pacing, etc.)." The plan: 1. Place temporary pacemaker 3.
CV, cardiovascular; HT, heart transplantation; ICU, intensive care unit; LVAD, left ventricular assist device. Aims Few studies have reported data on the optimal timing of left ventricular (LV) unloading during venoarterial extracorporeal membrane oxygenation (VA-ECMO) for cardiacarrest or shock.
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. (TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Lesions less than 70% are generally considered to be non-flow limiting. Two subsequent troponins were down trending.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. The described rhythm was an irregular, wide complex rhythm.
The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management CardiacArrest. See these other relevant cases: What are these bizarre bigeminal PVCs?? Is it STEMI?
Secondary endpoints included a composite of death, resuscitated cardiacarrest or implantation of another mechanical circulatory support device, duration of mechanical ventilation, and the length of intensive care unit (ICU) and hospital stays. The primary endpoint for this analysis was 1-year all-cause mortality.
He was admitted to the ICU and transferred emergently to a facility where he could undergo emergent dialysis as a part of further evaluation and management. Steve, what do you think of this ECG in this CardiacArrest Patient?" HyperKalemia with CardiacArrest. The QRS is narrow and T waves are much less peaked.
He was admitted to the ICU and was unstable, in shock, overnight. Case Continued: He was stabilized on more calcium, pressors, and high dose insulin. 3 hours later, this was recorded at a K of 2.8 mEq/L and total calcium of 14.7 mg/dL: The massive ST Elevation persists. What is going on here?
Fortunately, he was extubated several days later in the ICU with intact baseline mental status and was discharged shortly thereafter to subacute rehab. His troponin I peaked at 97 ng/mL (very large MI!). His follow up ECHO the next day revealed an EF of 24% and a posterior wall motion abnormality.
and the patient was given more insulin/dextrose/calcium and admitted to ICU. 2] Curiously, ACLS does not include consideration of calcium in its bradycardia algorithm, which could have prevented the arrest and which along with the epi produced ROSC. HyperKalemia with CardiacArrest. References 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content